

CyberKnife for hilar lung tumors: report of clinical response and toxicity
- PMID: 20969774
- PMCID: PMC2987864
- DOI: 10.1186/1756-8722-3-39
CyberKnife for hilar lung tumors: report of clinical response and toxicity
Abstract
Objective: To report clinical efficacy and toxicity of fractionated CyberKnife radiosurgery for the treatment of hilar lung tumors.
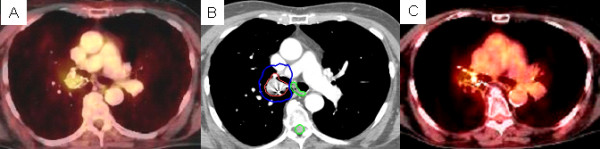
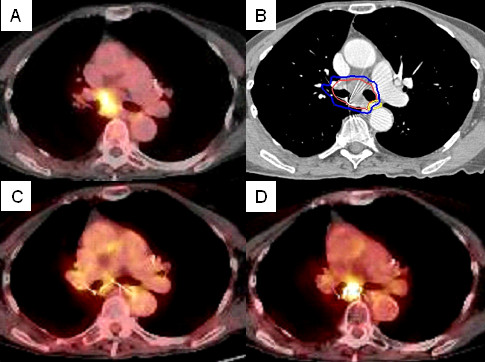
Methods: Patients presenting with primary and metastatic hilar lung tumors, treated using the CyberKnife system with Synchrony fiducial tracking technology, were retrospectively reviewed. Hilar location was defined as abutting or invading a mainstem bronchus. Fiducial markers were implanted by conventional bronchoscopy within or adjacent to tumors to serve as targeting references. A prescribed dose of 30 to 40 Gy to the gross tumor volume (GTV) was delivered in 5 fractions. Clinical examination and PET/CT imaging were performed at 3 to 6-month follow-up intervals.
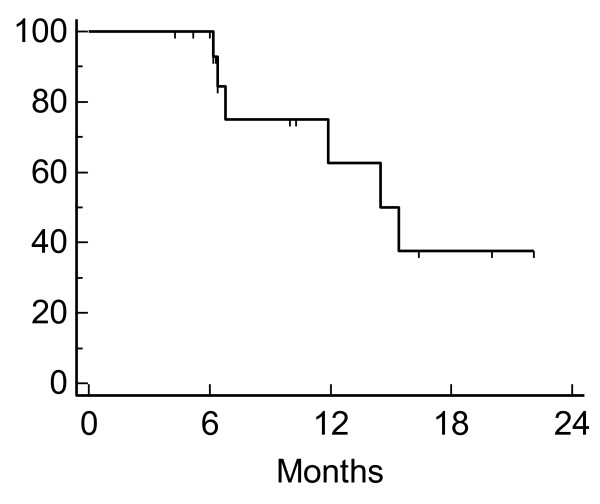
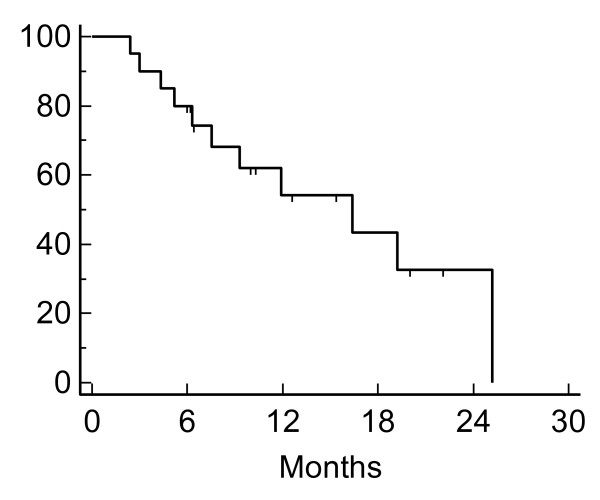
Results: Twenty patients were accrued over a 4 year period. Three had primary hilar lung tumors and 17 had hilar lung metastases. The median GTV was 73 cc (range 23-324 cc). The median dose to the GTV was 35 Gy (range, 30 - 40 Gy), delivered in 5 fractions over 5 to 8 days (median, 6 days). The resulting mean maximum point doses delivered to the esophagus and mainstem bronchus were 25 Gy (range, 11 - 39 Gy) and 42 Gy (range, 30 - 49 Gy), respectively. Of the 17 evaluable patients with 3 - 6 month follow-up, 4 patients had a partial response and 13 patients had stable disease. AAT t a median follow-up of 10 months, the 1-year Kaplan-Meier local control and overall survival estimates were 63% and 54%, respectively. Toxicities included one patient experiencing grade II radiation esophagitis and one patient experiencing grade III radiation pneumonitis. One patient with gross endobronchial tumor within the mainstem bronchus developed a bronchial fistula and died after receiving a maximum bronchus dose of 49 Gy.
Conclusion: CyberKnife radiosurgery is an effective palliative treatment option for hilar lung tumors, but local control is poor at one year. Maximum point doses to critical structures may be used as a guide for limiting toxicities. Preliminary results suggest that dose escalation alone is unlikely to enhance the therapeutic ratio of hilar lung tumors and novel approaches, such as further defining the patient population or employing the use of radiation sensitizers, should be investigated.
Figures
References
-
- Lax I, Panettieri V, Wennberg B, Amor Duch M, Naslund I, Baumann P, Gagliardi G. Dose distributions in SBRT of lung tumors: Comparison between two different treatment planning algorithms and Monte-Carlo simulation including breathing motions. Acta Oncol. 2006;45:978–988. doi: 10.1080/02841860600900050. - DOI - PubMed
-
- McGarry RC, Papiez L, Williams M, Whitford T, Timmerman RD. Stereotactic body radiation therapy of early-stage non-small-cell lung carcinoma: phase I study. Int J Radiat Oncol Biol Phys. 2005;63:1010–1015. - PubMed
-
- Timmerman R, McGarry R, Yiannoutsos C, Papiez L, Tudor K, DeLuca J, Ewing M, Abdulrahman R, DesRosiers C, Williams M, Fletcher J. Excessive toxicity when treating central tumors in a phase II study of stereotactic body radiation therapy for medically inoperable early-stage lung cancer. J Clin Oncol. 2006;24:4833–4839. doi: 10.1200/JCO.2006.07.5937. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
