

Predicting acute uncomplicated urinary tract infection in women: a systematic review of the diagnostic accuracy of symptoms and signs
- PMID: 20969801
- PMCID: PMC2987910
- DOI: 10.1186/1471-2296-11-78
Predicting acute uncomplicated urinary tract infection in women: a systematic review of the diagnostic accuracy of symptoms and signs
Abstract
Background: Acute urinary tract infections (UTI) are one of the most common bacterial infections among women presenting to primary care. However, there is a lack of consensus regarding the optimal reference standard threshold for diagnosing UTI. The objective of this systematic review is to determine the diagnostic accuracy of symptoms and signs in women presenting with suspected UTI, across three different reference standards (10(2) or 10(3) or 10(5) CFU/ml). We also examine the diagnostic value of individual symptoms and signs combined with dipstick test results in terms of clinical decision making.
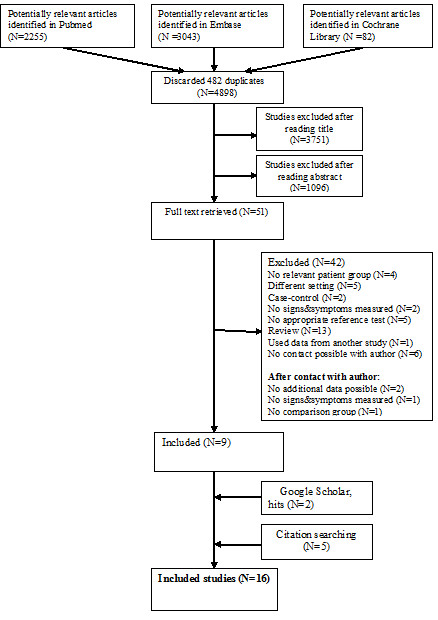
Methods: Searches were performed through PubMed (1966 to April 2010), EMBASE (1973 to April 2010), Cochrane library (1973 to April 2010), Google scholar and reference checking.Studies that assessed the diagnostic accuracy of symptoms and signs of an uncomplicated UTI using a urine culture from a clean-catch or catherised urine specimen as the reference standard, with a reference standard of at least ≥ 10(2) CFU/ml were included. Synthesised data from a high quality systematic review were used regarding dipstick results. Studies were combined using a bivariate random effects model.
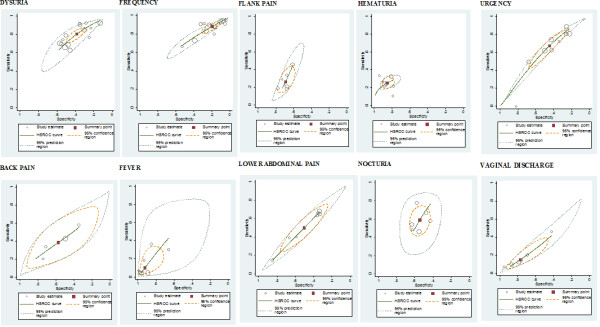
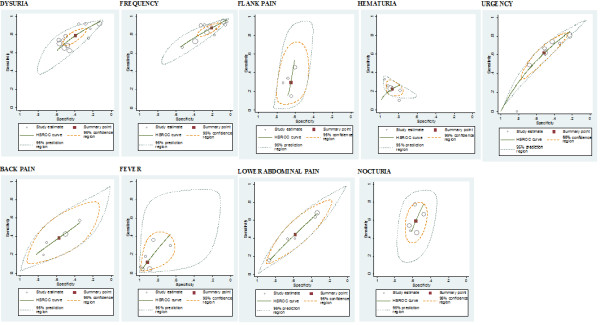
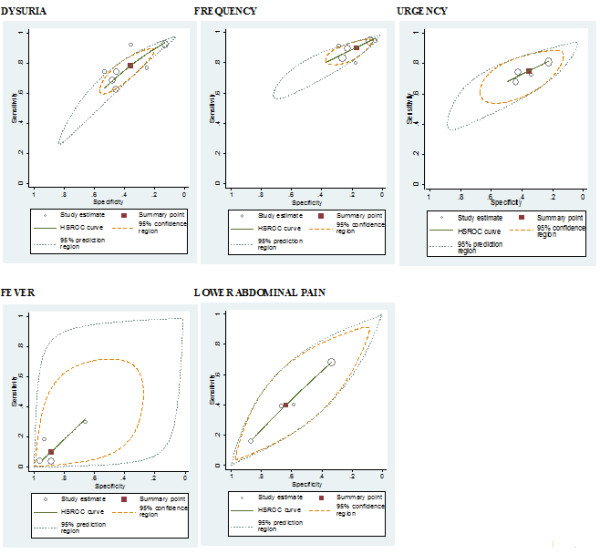
Results: Sixteen studies incorporating 3,711 patients are included. The weighted prior probability of UTI varies across diagnostic threshold, 65.1% at ≥ 10(2) CFU/ml; 55.4% at ≥ 10(3) CFU/ml and 44.8% at ≥ 10(2) CFU/ml ≥ 10(5) CFU/ml. Six symptoms are identified as useful diagnostic symptoms when a threshold of ≥ 10(2) CFU/ml is the reference standard. Presence of dysuria (+LR 1.30 95% CI 1.20-1.41), frequency (+LR 1.10 95% CI 1.04-1.16), hematuria (+LR 1.72 95%CI 1.30-2.27), nocturia (+LR 1.30 95% CI 1.08-1.56) and urgency (+LR 1.22 95% CI 1.11-1.34) all increase the probability of UTI. The presence of vaginal discharge (+LR 0.65 95% CI 0.51-0.83) decreases the probability of UTI. Presence of hematuria has the highest diagnostic utility, raising the post-test probability of UTI to 75.8% at ≥ 10(2) CFU/ml and 67.4% at ≥ 10(3) CFU/ml. Probability of UTI increases to 93.3% and 90.1% at ≥ 10(2) CFU/ml and ≥ 10(3) CFU/ml respectively when presence of hematuria is combined with a positive dipstick result for nitrites. Subgroup analysis shows improved diagnostic accuracy using lower reference standards ≥ 10(2) CFU/ml and ≥ 10(3) CFU/ml.
Conclusions: Individual symptoms and signs have a modest ability to raise the pretest-risk of UTI. Diagnostic accuracy improves considerably when combined with dipstick tests particularly tests for nitrites.
Figures
References
-
- Verheij R, Van Dijk C, Abrahamse H, Davids R, Vanden Hoogen H, Braspenning J, Landelijk Informatienetwerk Huisartsenzorg. Feiten en cijfers over huisartsenzorg in Nederland. Utrecht/Nijmegen. NIVEL/IQ. 2009. http://www.nivel.nl/oc2/page.asp?pageid=12694 bezocht op 6 september 2010.
-
- Kass EH. Asymptomatic infections of the urinary tract. Trans Assoc Am Physicians. 1956;69:56–64. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
