

Transapical aortic valve replacement under real-time magnetic resonance imaging guidance: experimental results with balloon-expandable and self-expanding stents
- PMID: 20971017
- PMCID: PMC3038190
- DOI: 10.1016/j.ejcts.2010.09.030
Transapical aortic valve replacement under real-time magnetic resonance imaging guidance: experimental results with balloon-expandable and self-expanding stents
Abstract
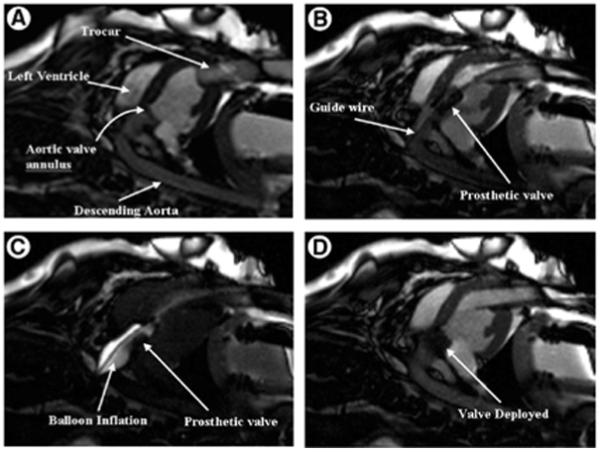
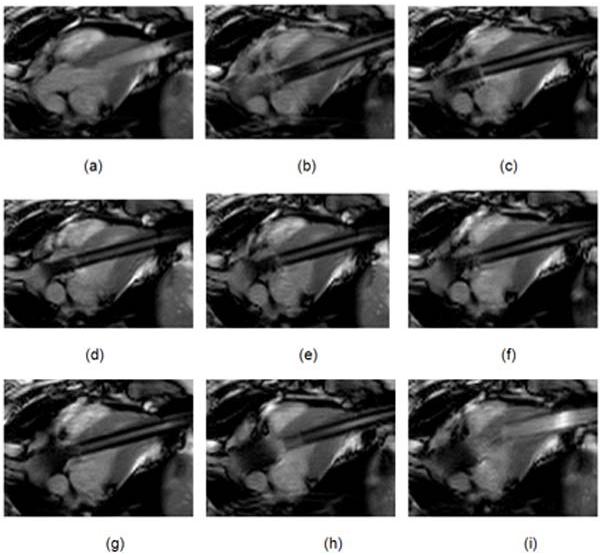
Objective: Aortic valves have been implanted on self-expanding (SE) and balloon-expandable (BE) stents minimally invasively. We have demonstrated the advantages of transapical aortic valve implantation (tAVI) under real-time magnetic resonance imaging (rtMRI) guidance. Whether there are different advantages to SE or BE stents is unknown. We report rtMRI-guided tAVI in a porcine model using both SE and BE stents, and compare the differences between the stents.
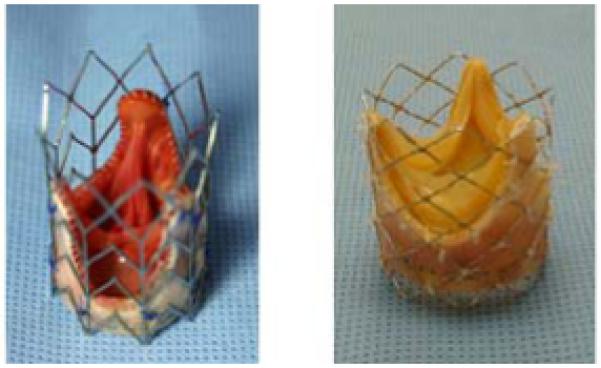
Methods: A total of 22 Yucatan pigs (45-57 kg) underwent tAVI. Commercially available stentless bioprostheses (21-25 mm) were mounted on either BE platinum-iridium stents or SE-nitinol stents. rtMRI guidance was employed as the intraoperative imaging. Markers on both types of stents were used to enhance visualization in rtMRI. Pigs were allowed to survive and had follow-up MRI scans and echocardiography at 1, 3, and 6 months postoperatively.
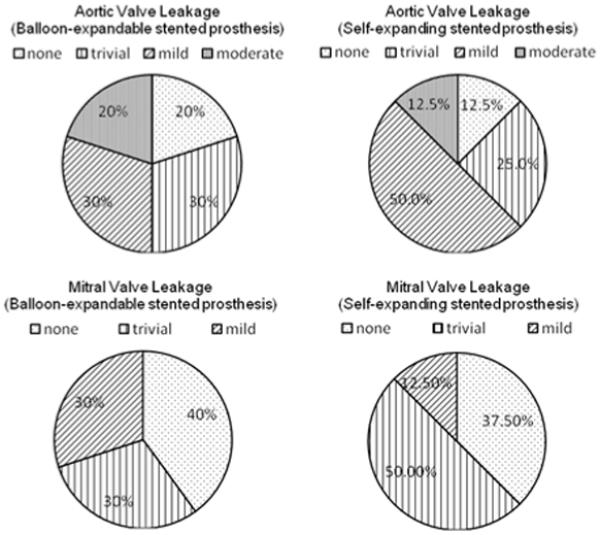
Results: rtMRI provided excellent visualization of the aortic valve implantation mounted on both stent types. The implantation times were shorter with the SE stents (60 ± 14s) than with the BE stents (74 ± 18s), (p=0.027). The total procedure time was 31 and 37 min, respectively (p=0.12). It was considerably easier to manipulate the SE stent during deployment, without hemodynamic compromise. This was not always the case with the BE stent, and its placement occasionally resulted in coronary obstruction and death. Long-term results demonstrated stability of the implants with preservation of myocardial perfusion and function over time for both stents.
Conclusions: SE stents were easier to position and deploy, thus leading to fewer complications during tAVI. Future optimization of SE stent design should improve clinical results.
Copyright © 2010 European Association for Cardio-Thoracic Surgery. All rights reserved.
Figures



References
-
- Lutter G, Kuklinski D, Berg G, Von Samson P, Martin J, Handke M, Uhrmeister P, Beyersdorf F. Percutaneous aortic valve replacement: an experimental study. I. Studies on implantation. J Thorac Cardiovasc Surg. 2002;123(4):768–776. - PubMed
-
- Kuehne T, Yilmaz S, Meinus C, Moore P, Saeed M, Weber O, Higgins CB, Blank T, Elsaesser E, Schnackenburg B, Ewert P, Lange PE, Nagel E. Magnetic resonance imaging-guided transcatheter implantation of a prosthetic valve in aortic valve position: feasibility study in swine. J Am Coll Cardiol. 2004;44(11):2247–58. - PubMed
-
- Grube E, Laborde JC, Zickmann B, Gerckens U, Felderhoff T, Sauren B, Bootsveld A, Buellesfeld L, Iversen S. First report on a human percutaneous transluminal implantation of a self-expanding valve prosthesis for interventional treatment of aortic valve stenosis. Catheter Cardiovasc Interv. 2005;66:465–469. - PubMed
-
- Hanzel GS, Harrity PJ, Schreiber TL, O’Neill WW. Retrograde percutaneous aortic valve implantation for critical aortic stenosis. Catheter Cardiovasc Interv. 2005;64:322–326. - PubMed
-
- Cribier A, Eltchaninoff H, Tron C, Bauer F, Agatiello C, Nercolini D, Tapiero S, Litzler P, Bessou J, Babaliaros V. Treatment of calcific aortic stenosis with the percutaneous heart Valve: mid-term follow-up from the initial feasibility studies: the french experience. J Am Coll Cardiol. 2006;47(6):1214–1223. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
