

Influence of patient age on procedural selection in mitral valve surgery
- PMID: 20971244
- PMCID: PMC4322678
- DOI: 10.1016/j.athoracsur.2010.05.075
Influence of patient age on procedural selection in mitral valve surgery
Abstract
Background: Previous studies suggest that mitral valve replacement is comparable to repair in the elderly, and a national trend exists toward tissue valves. However, few direct comparison data are available, and this study evaluated the effects of patient age on risk-adjusted survival after mitral procedures.
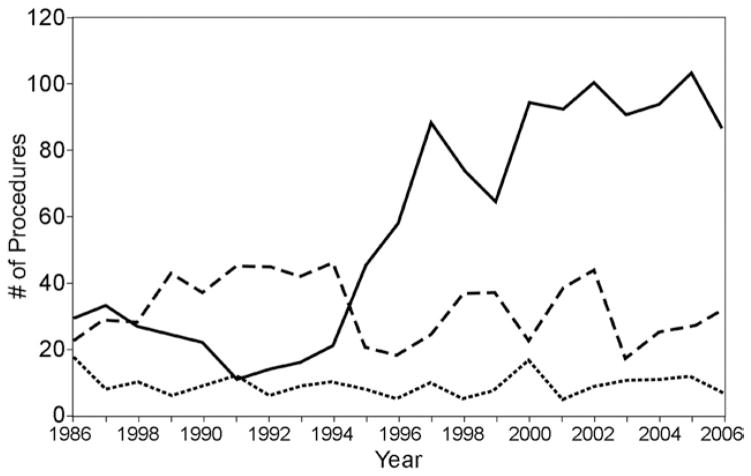
Methods: From 1986 to 2006, 2,064 patients underwent isolated primary mitral operations (±CABG). Maximal follow-up was 20 years with a median of 5 years. Valve disease etiology was the following: degenerative, 864; ischemic, 450; rheumatic, 416; endocarditis, 98; and "other," 236. Overall, 58% had repair and 39% had concomitant coronary artery bypass grafting. Survival differences were evaluated with a Cox proportional hazards model that included baseline characteristics, valve disease etiology, and choice of repair versus replacement with tissue or mechanical valves.
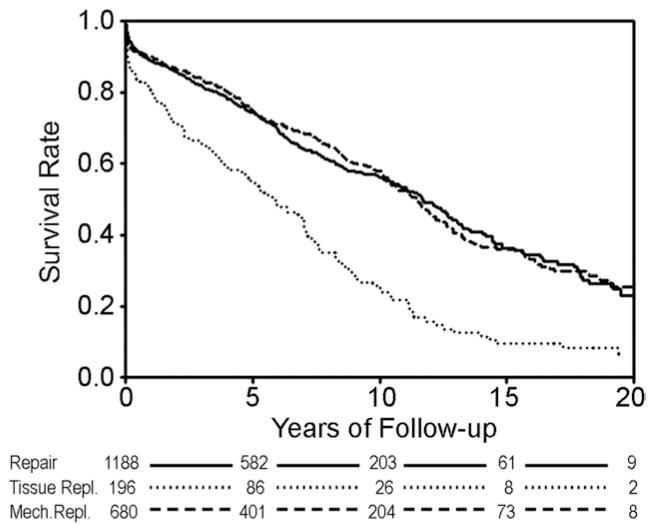
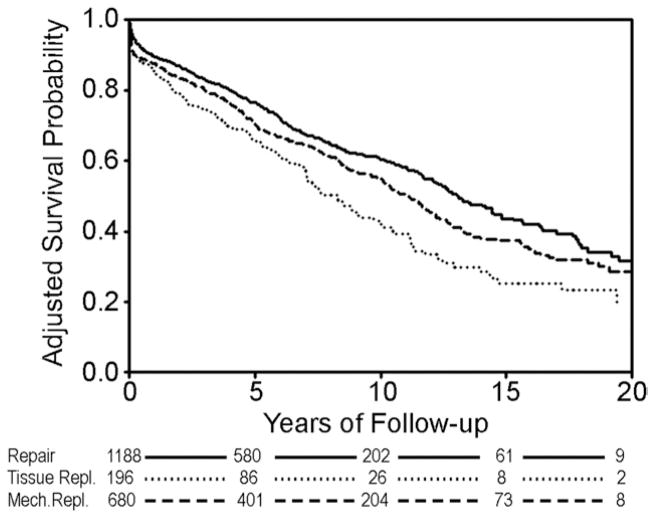
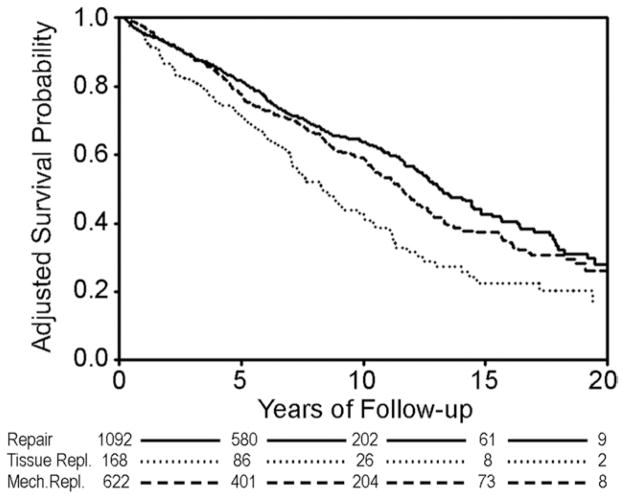
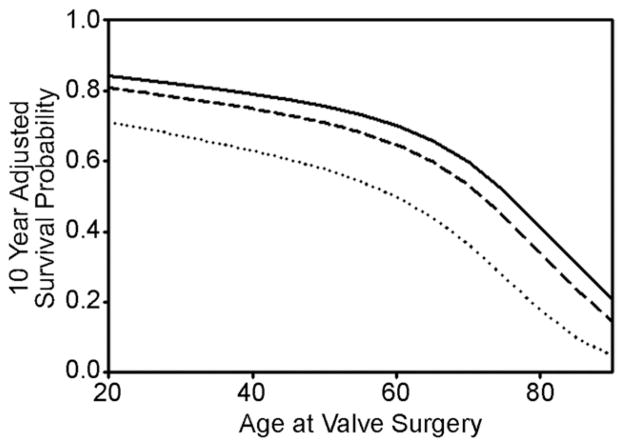
Results: Baseline risk profiles generally were better for mechanical valves, and age was the most significant multivariable predictor of late mortality [hazard ratio = 1.4 per 10-year increment, Wald χ(2) = 32.7, p < 0.0001]. As compared with repair, risk-adjusted survival was inferior with either tissue valves [1.8, 27.6, <0.0001] or mechanical valves [1.3, 8.1, 0.0044], and no treatment interaction was observed with age (p = 0.18). At no patient age did tissue valves achieve equivalent survival to either repair or mechanical valves.
Conclusions: Mitral repair is associated with better survival than valve replacement across the spectrum of patient age. If replacement is required, mechanical valves achieve better outcomes, even in the elderly. These data suggest that tissue valves should be reserved only for patients with absolute contraindications to anticoagulation who are not amenable to repair.
Copyright © 2010 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Lawrie GM, Earle EA, Earle NR. Feasibility and intermediate term outcome of repair of prolapsing anterior mitral leaflets with artificial chordal replacement in 152 patients. Ann Thorac Surg. 2006;81:849–56. - PubMed
-
- Chauvaud S, Jebara V, Chachques JC, et al. Valve extension with glutaraldehyde-preserved autologous pericardium. Results in mitral valve repair. J Thorac Cardiovasc Surg. 1991;102:171–7. - PubMed
-
- Rankin JS. Artificial chordal replacement in complex mitral valve repair. Available at CTSNet: http://www.ctsnet.org/sections/clinicalresources/videos/vg2009_rankin_AC....
-
- Rankin JS, Alfery DD, Orozco R, et al. Techniques of artificial chordal replacement for mitral valve repair: Use in multiple pathologic disorders. Op Tech Thorac Cardiovasc Surg. 2008;13:74–82.
-
- Ailawadi G, MD, Swenson BR, Girotti ME. Is mitral valve repair superior to replacement in elderly patients? Ann Thorac Surg. 2008;86:77–86. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
