

The cerebrovascular dysfunction induced by slow pressor doses of angiotensin II precedes the development of hypertension
- PMID: 20971763
- PMCID: PMC3023263
- DOI: 10.1152/ajpheart.00679.2010
The cerebrovascular dysfunction induced by slow pressor doses of angiotensin II precedes the development of hypertension
Abstract
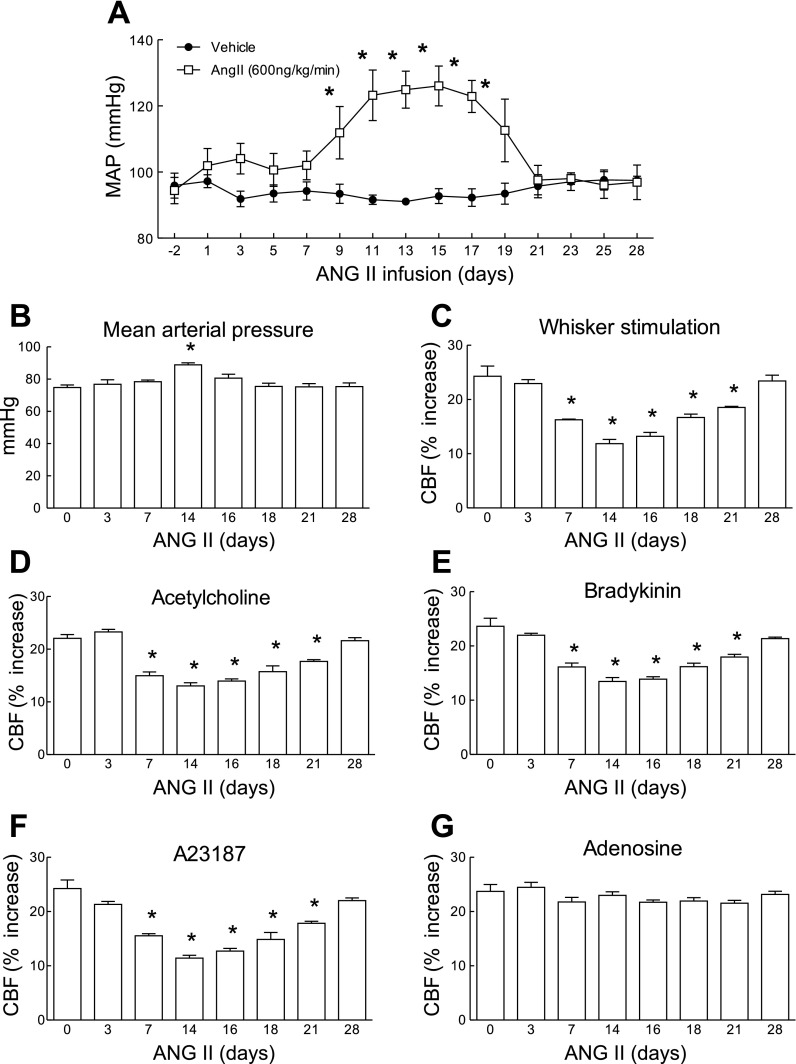
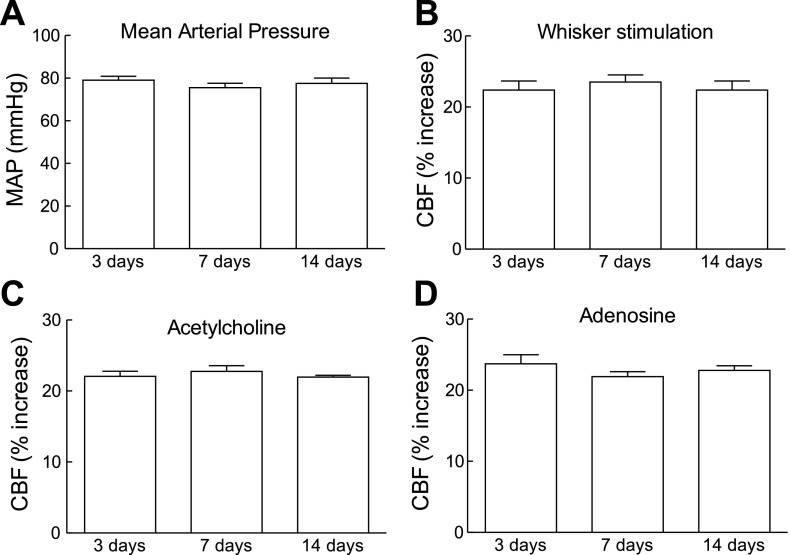
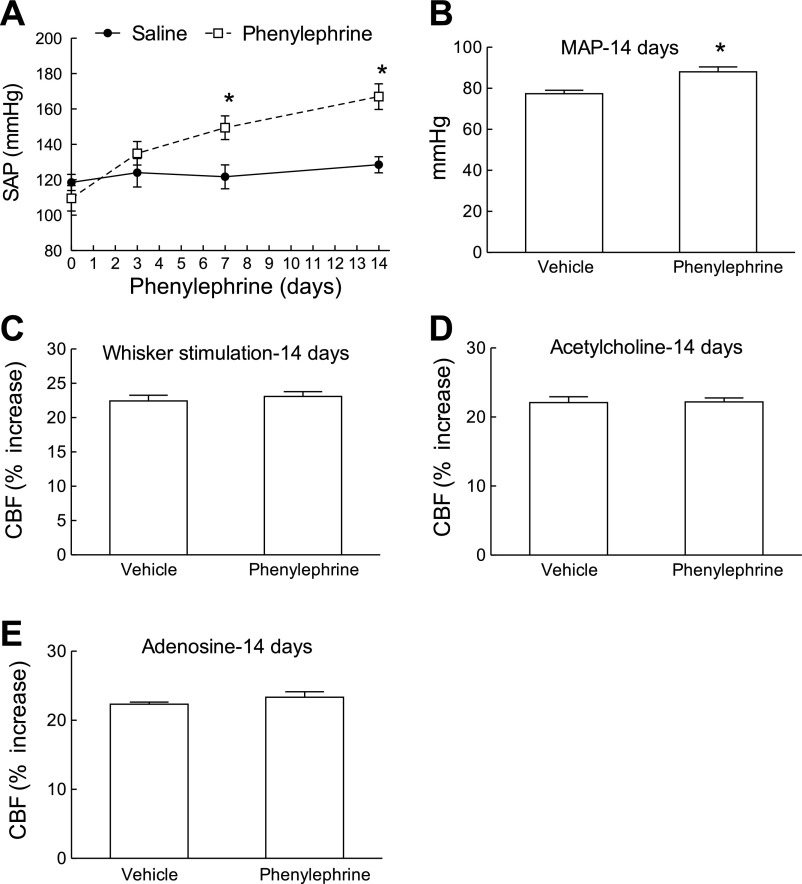
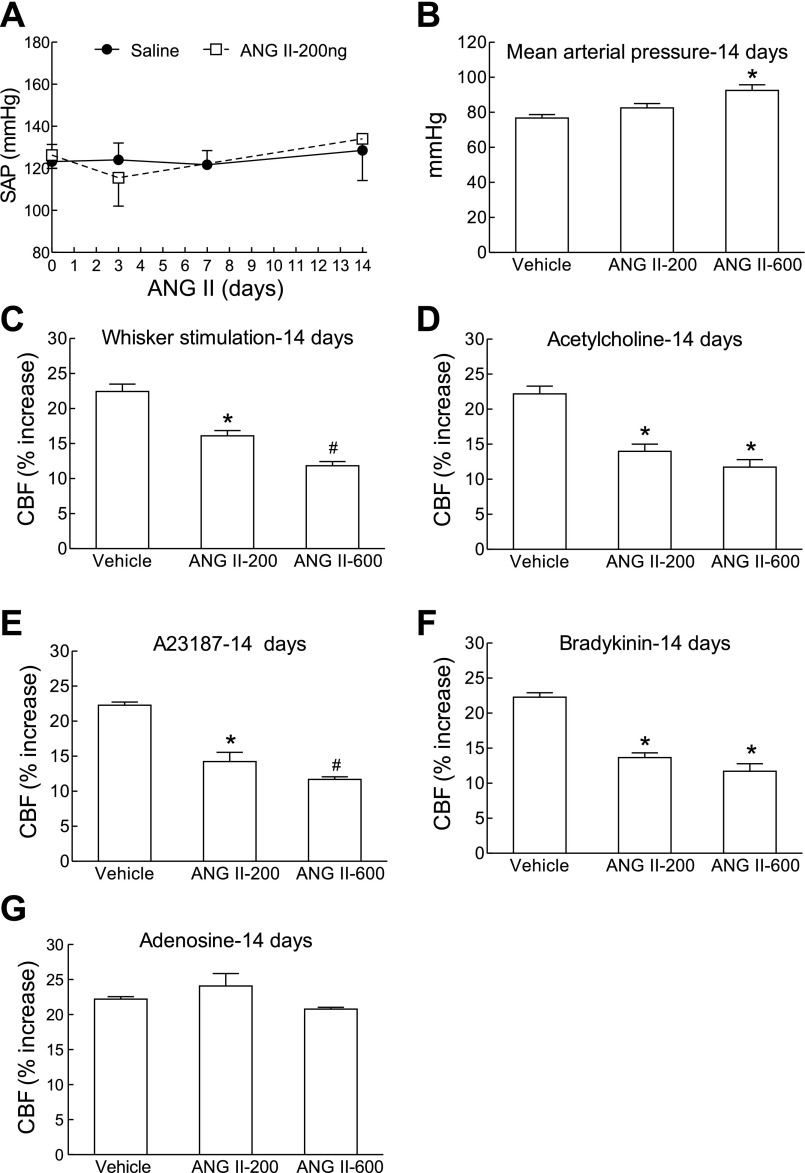
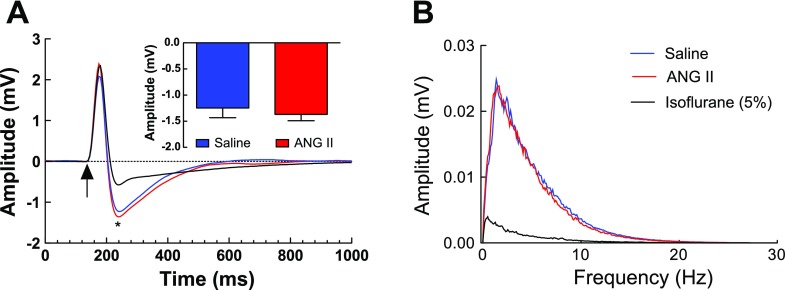
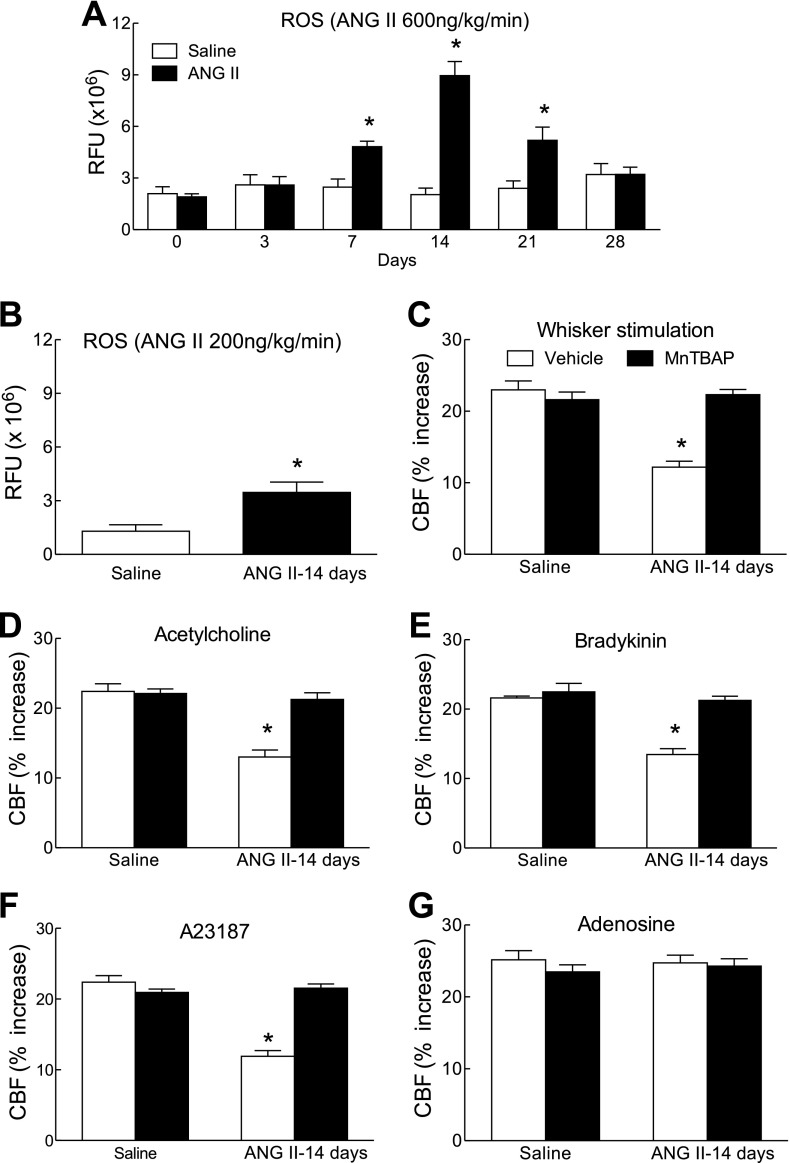
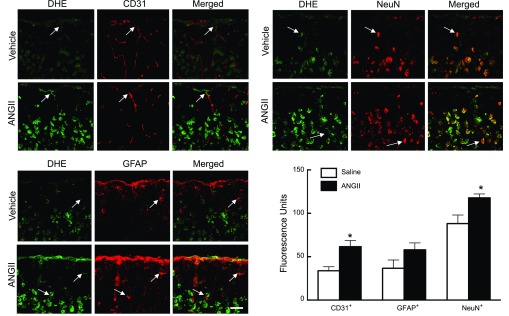
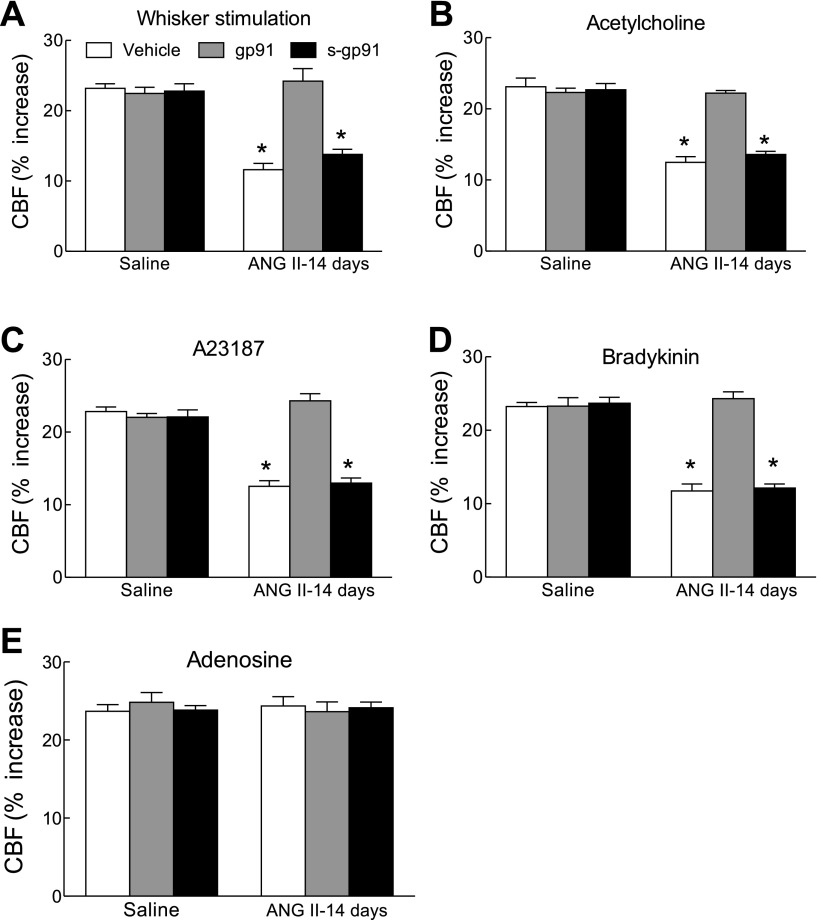
Hypertension alters cerebrovascular regulation and increases the brain's susceptibility to stroke and dementia. We investigated the temporal relationships between the arterial pressure (AP) elevation induced by "slow pressor" angiotensin II (ANG II) infusion, which recapitulates key features of human hypertension, and the resulting cerebrovascular dysfunction. Minipumps delivering saline or ANG II for 14 days were implanted subcutaneously in C57BL/6 mice (n = 5/group). Cerebral blood flow was assessed by laser-Doppler flowmetry in anesthetized mice equipped with a cranial window. With ANG II (600 ng · kg(-1) · min(-1)), AP started to rise after 9 days (P < 0.05 vs. saline), remained elevated at 11-17 days, and returned to baseline at 21 days (P > 0.05). ANG II attenuated the cerebral blood flow increase induced by neural activity (whisker stimulation) or endothelium-dependent vasodilators, an effect observed before the AP elevation (7 days), as well as after the hypertension subsided (21 days). Nonpressor doses of ANG II (200 ng · kg(-1) · min(-1)) induced cerebrovascular dysfunction and oxidative stress without elevating AP (P > 0.05 vs. saline), whereas phenylephrine elevated AP without inducing cerebrovascular effects. ANG II (600 ng · kg(-1) · min(-1)) augmented neocortical reactive oxygen species (ROS) with a time course similar to that of the cerebrovascular dysfunction. Neocortical application of the ROS scavenger manganic(I-II)meso-tetrakis(4-benzoic acid)porphyrin or the NADPH oxidase peptide inhibitor gp91ds-tat attenuated ROS and cerebrovascular dysfunction. We conclude that the alterations in neurovascular regulation induced by slow pressor ANG II develop before hypertension and persist beyond AP normalization but are not permanent. The findings unveil a striking susceptibility of cerebrovascular function to the deleterious effects of ANG II and raise the possibility that cerebrovascular dysregulation precedes the elevation in AP also in patients with ANG II-dependent hypertension.
Figures
References
-
- Andresen J, Shafi NI, Bryan RM., Jr Endothelial influences on cerebrovascular tone. J Appl Physiol 100:318–327, 2006. - PubMed
-
- Benarroch EE. Paraventricular nucleus, stress response, and cardiovascular disease. Clin Auton Res 15:254–263, 2005. - PubMed
-
- Butz GM, Davisson RL. Long-term telemetric measurement of cardiovascular parameters in awake mice: a physiological genomics tool. Physiol Genomics 5:89–97, 2001. - PubMed
-
- Chobanian A, Bakris G, Black H, Cushman W, Green L, Izzo J, Jones D, Materson B, Oparil S, Wright J, Roccella E. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 289:2560–2572, 2003. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous