

Differentiating chronic lymphocytic leukemia from monoclonal B-lymphocytosis according to clinical outcome: on behalf of the GIMEMA chronic lymphoproliferative diseases working group
- PMID: 20971821
- PMCID: PMC3031696
- DOI: 10.3324/haematol.2010.030189
Differentiating chronic lymphocytic leukemia from monoclonal B-lymphocytosis according to clinical outcome: on behalf of the GIMEMA chronic lymphoproliferative diseases working group
Abstract
Background: Optimal lymphocyte parameters and thresholds for the diagnosis of chronic lymphocytic leukemia have been proposed by The National Cancer Institute sponsored Working Group and recently updated by the International Workshop on chronic lymphocytic leukemia. However, it is not clear how these criteria apply to patient management in daily clinical practice and whether the lymphocyte thresholds recommended truly predict clinical outcome in early chronic lymphocytic leukemia.
Design and methods: For the purpose of this study, an observational database of the GIMEMA (Gruppo Italiano Malattie Ematologiche dell'Adulto) which included 1,158 patients with newly diagnosed Binet stage A chronic lymphocytic leukemia who were observed at different primary hematology centers during the period 1991-2000, was used.
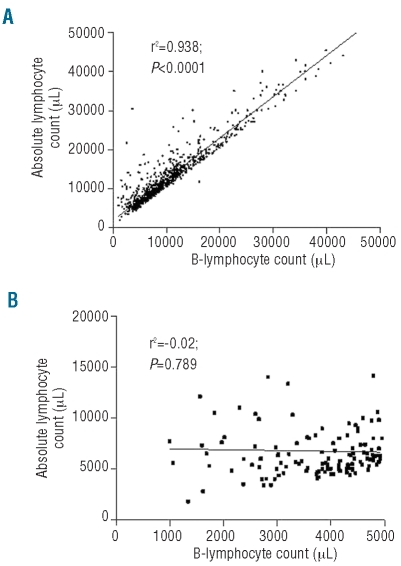
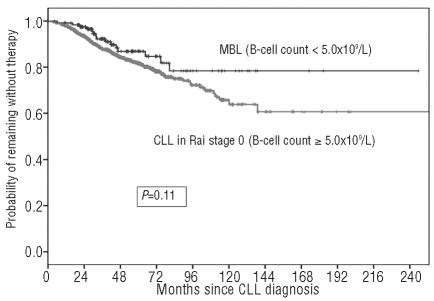
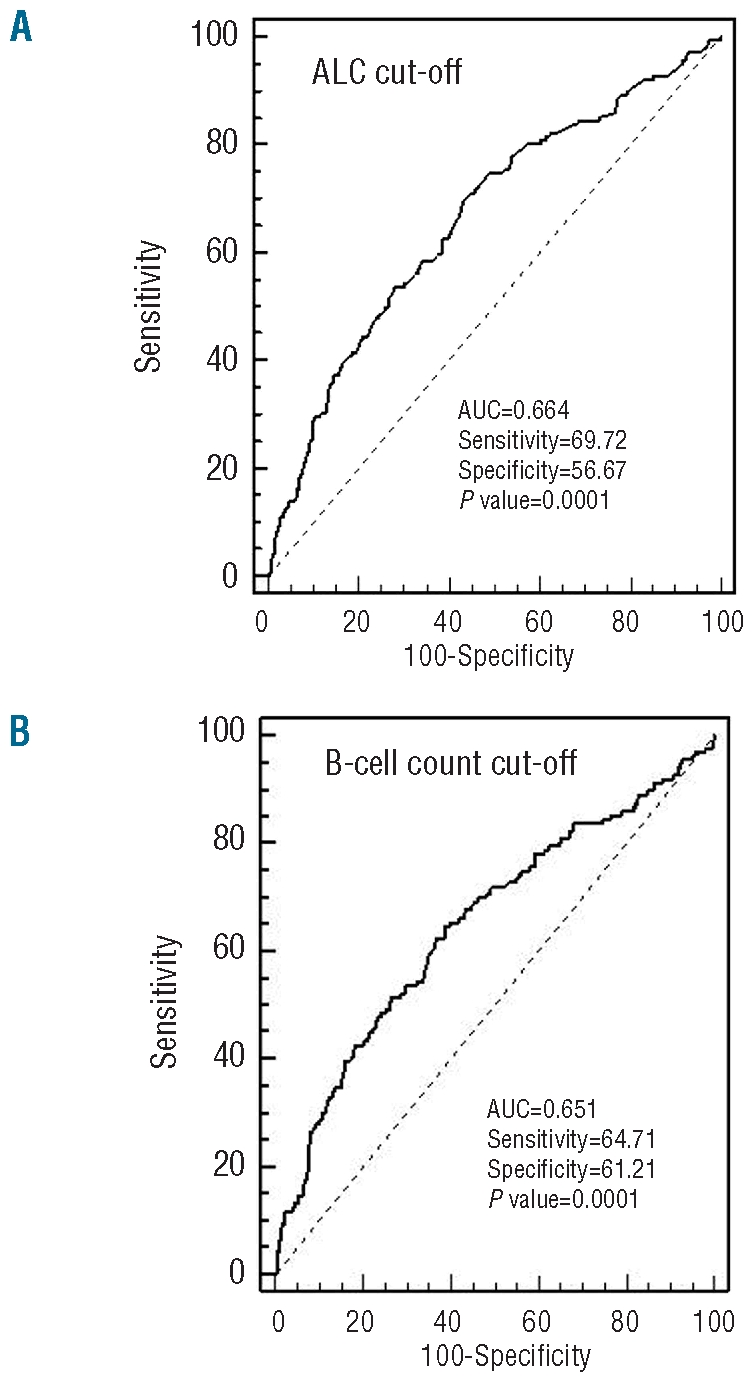
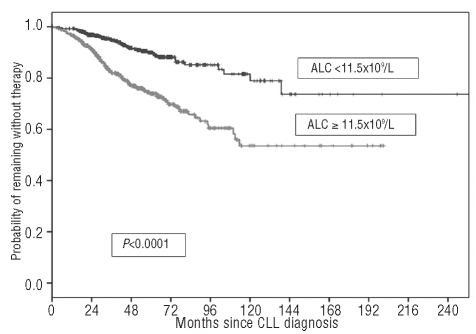
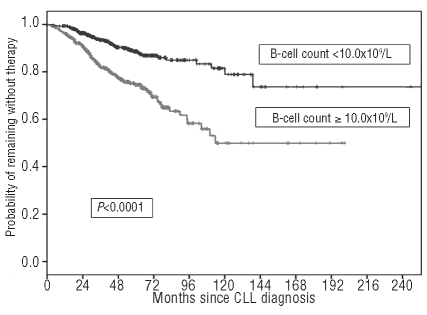
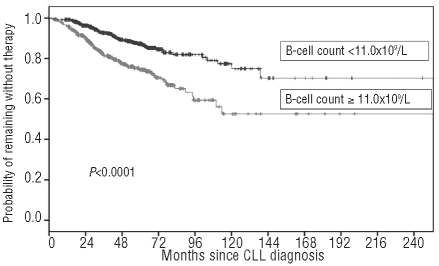
Results: Among 818 consecutive chronic lymphocytic leukemia patients with Rai stage 0 (i.e. no palpable lymphadenopathy or hepatosplenomegaly) who had flow cytometry evaluations at the time of diagnosis and were included in a GIMEMA database, both absolute lymphocyte count and B-cell count were of a similar value in predicting time to first treatment as continuous variables (P<0.0001). Receiver operating characteristic analysis identified an absolute lymphocyte count of 11.5×10(9)/L and an absolute B-cell count of 10.0×10(9)/L as the best thresholds capable of identifying patients who will require treatment from those with stable disease. However, in a Cox's multivariate analysis only the B-cell count retained its discriminating power (P<0.0001) and the estimated rate of progression to chronic lymphocytic leukemia requiring treatment among subjects with a B-cell count less than 10.0×10(9)/L was approximately 2.3% per year (95% CI 2.1-2.5%) while it was 2-fold higher for patients with a B-cell count of 10.0×10(9)/L or over (i.e. 5.2% per year; 95% CI 4.9-5.5%). Finally, in this community-based patient cohort, the B-cell threshold defined by investigators at the Mayo Clinic (i.e. 11.0×10(9)/L) allowed patients to be divided into two subsets with a higher and lower likelihood of treatment (P<0.0001).
Conclusions: Our results, based on a retrospective patients' cohort, provide a clear justification to retain the B-cell count as the reference gold standard of chronic lymphocytic leukemia diagnosis and imply that a count of 10×10(9)/L B cells is the best lymphocyte threshold to predict time to first treatment. The use of clinical outcome to distinguish chronic lymphocytic leukemia from other premalignant conditions, such as monoclonal B-cell lymphocytosis, is a pragmatic approach meeting the patients' need to minimize the psychological discomfort of receiving a diagnosis of leukemia when the risk of adverse clinical consequences is low.
Figures
Similar articles
-
Incidence of chronic lymphocytic leukemia and high-count monoclonal B-cell lymphocytosis using the 2008 guidelines.Cancer. 2014 Jul 1;120(13):2000-5. doi: 10.1002/cncr.28690. Epub 2014 Apr 7. Cancer. 2014. PMID: 24711224 Free PMC article.
-
B-cell count and survival: differentiating chronic lymphocytic leukemia from monoclonal B-cell lymphocytosis based on clinical outcome.Blood. 2009 Apr 30;113(18):4188-96. doi: 10.1182/blood-2008-09-176149. Epub 2008 Nov 17. Blood. 2009. PMID: 19015397 Free PMC article.
-
The utility of a prognostic index for predicting time to first treatment in early chronic lymphocytic leukemia: the GIMEMA experience.Haematologica. 2010 Mar;95(3):464-9. doi: 10.3324/haematol.2009.011767. Epub 2009 Nov 10. Haematologica. 2010. PMID: 19903673 Free PMC article.
-
Monoclonal B-cell lymphocytosis: Does the elderly patient need a specialistic approach?Eur J Intern Med. 2018 Dec;58:2-6. doi: 10.1016/j.ejim.2018.09.006. Epub 2018 Sep 26. Eur J Intern Med. 2018. PMID: 30268574 Review.
-
Monoclonal B-cell lymphocytosis and early-stage chronic lymphocytic leukemia: diagnosis, natural history, and risk stratification.Blood. 2015 Jul 23;126(4):454-62. doi: 10.1182/blood-2015-02-585059. Epub 2015 Jun 11. Blood. 2015. PMID: 26065657 Free PMC article. Review.
Cited by
-
A prognostic algorithm including a modified version of MD Anderson Cancer Center (MDACC) score predicts time to first treatment of patients with clinical monoclonal lymphocytosis (cMBL)/Rai stage 0 chronic lymphocytic leukemia (CLL).Int J Hematol. 2014 Sep;100(3):290-5. doi: 10.1007/s12185-014-1634-7. Epub 2014 Jul 27. Int J Hematol. 2014. PMID: 25064370 Clinical Trial.
-
Prevalence of monoclonal B lymphocytosis in first-degree relatives of chronic lymphocytic leukemia patients in Turkey.Turk J Haematol. 2015 Mar 5;32(1):29-34. doi: 10.4274/tjh.2013.0288. Turk J Haematol. 2015. PMID: 25805672 Free PMC article.
-
Incidence of chronic lymphocytic leukemia and high-count monoclonal B-cell lymphocytosis using the 2008 guidelines.Cancer. 2014 Jul 1;120(13):2000-5. doi: 10.1002/cncr.28690. Epub 2014 Apr 7. Cancer. 2014. PMID: 24711224 Free PMC article.
-
The 2008 WHO classification of lymphoid neoplasms and beyond: evolving concepts and practical applications.Blood. 2011 May 12;117(19):5019-32. doi: 10.1182/blood-2011-01-293050. Epub 2011 Feb 7. Blood. 2011. PMID: 21300984 Free PMC article. Review.
-
HLA specificities are associated with prognosis in IGHV-mutated CLL-like high-count monoclonal B cell lymphocytosis.PLoS One. 2017 Mar 1;12(3):e0172978. doi: 10.1371/journal.pone.0172978. eCollection 2017. PLoS One. 2017. PMID: 28249016 Free PMC article.
References
-
- Rozman C, Bosch F, Montserrat E. Chronic lymphocytic leukemia: a changing natural history? Leukemia. 1997;11(6):775–8. - PubMed
-
- Molica S, Levato D. What is changing in the natural history of chronic lymphocytic leukemia. Haematologica. 2001;86(1):8–12. - PubMed
-
- Abrisqueta P, Pereira A, Rozman C, Aymerich M, Gine E, Moreno C, et al. Improving survival in patients with chronic lymphocytic leukemia (1980–2008): the Hospital Clinic of Barcelona experience. Blood. 2009;114(10):2044–50. - PubMed
-
- Cheson BD, Bennett JM, Grever M, Kay N, Keating MJ, O’Brien S, Rai KR. National Cancer Institute-sponsored Working Group guidelines for chronic lymphocytic leukemia: revised guidelines for diagnosis and treatment. Blood. 1996;87(12):4990–7. - PubMed
-
- Marti GE, Rawstron AC, Ghia P, Hillmen P, Houlston RS, Kay N, et al. Diagnostic criteria for monoclonal B-cell lymphocytosis. Br J Haematol. 2005;130(3):325–32. - PubMed
