

Late onset sporadic dilated cardiomyopathy caused by a cardiac troponin T mutation
- PMID: 20973921
- PMCID: PMC2965560
- DOI: 10.1111/j.1752-8062.2010.00228.x
Late onset sporadic dilated cardiomyopathy caused by a cardiac troponin T mutation
Abstract
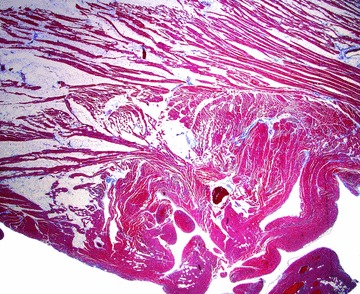
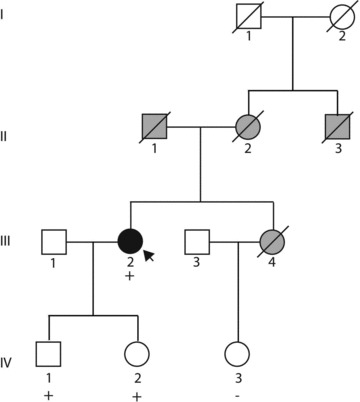
Mutations in TNNT2, encoding cardiac troponin T, commonly shows early onset, aggressive dilated cardiomyopathy (DCM). This observation may influence the decision of whether to undertake clinical genetic testing for TNNT2 in later onset DCM. Further, the trigger for late onset DCM remains enigmatic. A 70-year-old woman, previously healthy with a left ventricular ejection fraction of 50%-55% at age 69, presented with DCM of unknown cause and a 4-month history progressive heart failure requiring cardiac transplantation. Clinical genetic testing revealed a novel TNNT2 R139H mutation but no relevant variants in 18 other DCM genes. Her explanted heart showed partial fatty replacement in the right ventricle. Sequencing for five arrhythmogenic right ventricular dysplasia genes was negative. Functional studies in porcine cardiac skinned fibers reconstituted with the mutant R139H troponin T protein showed decreased Ca(2+) sensitivity at pH 7, characteristic of DCM. Because fatty infiltration may acidify the myocellular environment, maximal force development examined at pH 6.5 was diminished, suggesting a possible environmental trigger. We conclude that the TNNT2 R139H mutation was likely to be disease causing. Further, later age of onset may not be relevant to exclude genetic testing for TNNT2 mutations.
© 2010 Wiley Periodicals, Inc.
Figures


Similar articles
-
Clinical and functional characterization of TNNT2 mutations identified in patients with dilated cardiomyopathy.Circ Cardiovasc Genet. 2009 Aug;2(4):306-13. doi: 10.1161/CIRCGENETICS.108.846733. Epub 2009 May 15. Circ Cardiovasc Genet. 2009. PMID: 20031601 Free PMC article.
-
Novel Genetic Variants in BAG3 and TNNT2 in a Swedish Family with a History of Dilated Cardiomyopathy and Sudden Cardiac Death.Pediatr Cardiol. 2017 Aug;38(6):1262-1268. doi: 10.1007/s00246-017-1655-0. Epub 2017 Jul 1. Pediatr Cardiol. 2017. PMID: 28669108 Free PMC article.
-
Severe disease expression of cardiac troponin C and T mutations in patients with idiopathic dilated cardiomyopathy.J Am Coll Cardiol. 2004 Nov 16;44(10):2033-40. doi: 10.1016/j.jacc.2004.08.027. J Am Coll Cardiol. 2004. PMID: 15542288
-
[Genetics of dilated cardiomyopathy].Z Kardiol. 2001 Jul;90(7):461-9. doi: 10.1007/s003920170134. Z Kardiol. 2001. PMID: 11515275 Review. German.
-
[Mutations in genes for sarcomeric proteins].Nihon Rinsho. 2000 Jan;58(1):117-22. Nihon Rinsho. 2000. PMID: 10885298 Review. Japanese.
Cited by
-
Exome Sequencing Identifies Pathogenic and Modifier Mutations in a Child With Sporadic Dilated Cardiomyopathy.J Am Heart Assoc. 2015 Dec 9;4(12):e002443. doi: 10.1161/JAHA.115.002443. J Am Heart Assoc. 2015. PMID: 26656454 Free PMC article.
-
Focus on cardiac troponin complex: From gene expression to cardiomyopathy.Genes Dis. 2024 Mar 11;11(6):101263. doi: 10.1016/j.gendis.2024.101263. eCollection 2024 Nov. Genes Dis. 2024. PMID: 39211905 Free PMC article. Review.
-
Contractility of ventricular myocytes is well preserved despite altered mechanisms of Ca2+ transport and a changing pattern of mRNA in aged type 2 Zucker diabetic fatty rat heart.Mol Cell Biochem. 2012 Feb;361(1-2):267-80. doi: 10.1007/s11010-011-1112-y. Epub 2011 Oct 19. Mol Cell Biochem. 2012. PMID: 22009485
-
Return of genetic results in the familial dilated cardiomyopathy research project.J Genet Couns. 2013 Apr;22(2):164-74. doi: 10.1007/s10897-012-9532-8. Epub 2012 Aug 11. J Genet Couns. 2013. PMID: 22886719 Free PMC article.
-
Genetic evaluation of dilated cardiomyopathy.Curr Cardiol Rep. 2013 Jul;15(7):375. doi: 10.1007/s11886-013-0375-1. Curr Cardiol Rep. 2013. PMID: 23686784 Review.
References
-
- Hershberger RE, Lindenfeld J, Mestroni L, Seidman CE, Taylor MR, Towbin JA. Genetic evaluation of cardiomyopathy—a Heart Failure Society of America practice guideline. J Card Fail. 2009; 15: 83–97. - PubMed
-
- Burkett EL, Hershberger RE. Clinical and genetic issues in familial dilated cardiomyopathy. J Am Coll Cardiol. 2005; 45: 969–981. - PubMed
-
- Hershberger RE, Kushner JK, Parks SP. Dilated Cardiomyopathy Overview. In: GeneReviews at GeneTests: Medical Genetics Information Resource (database online). Available at: http://www.genetests.org. Accessed July 10, 2008.
-
- Judge DP, Johnson NM. Genetic evaluation of familial cardiomyopathy. J Cardiovasc Trans Res. 2008; 1: 144–154. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
