

Defining human mesenchymal stem cell efficacy in vivo
- PMID: 20974000
- PMCID: PMC2987779
- DOI: 10.1186/1476-9255-7-51
Defining human mesenchymal stem cell efficacy in vivo
Abstract
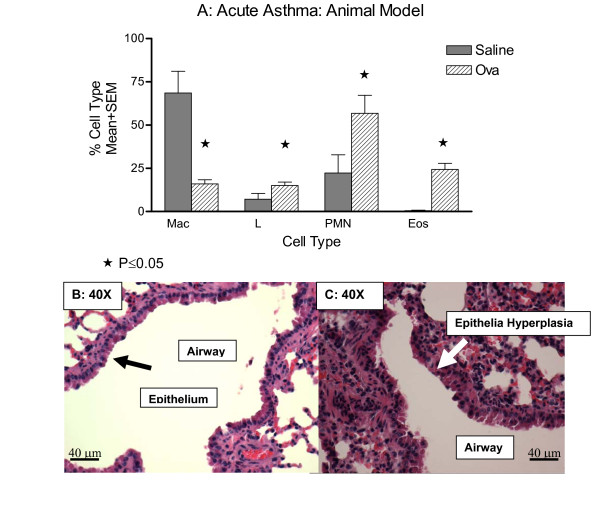
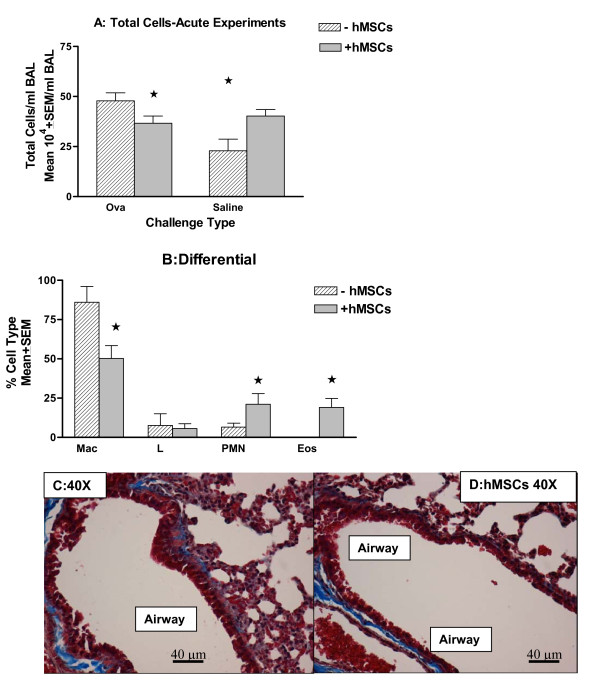
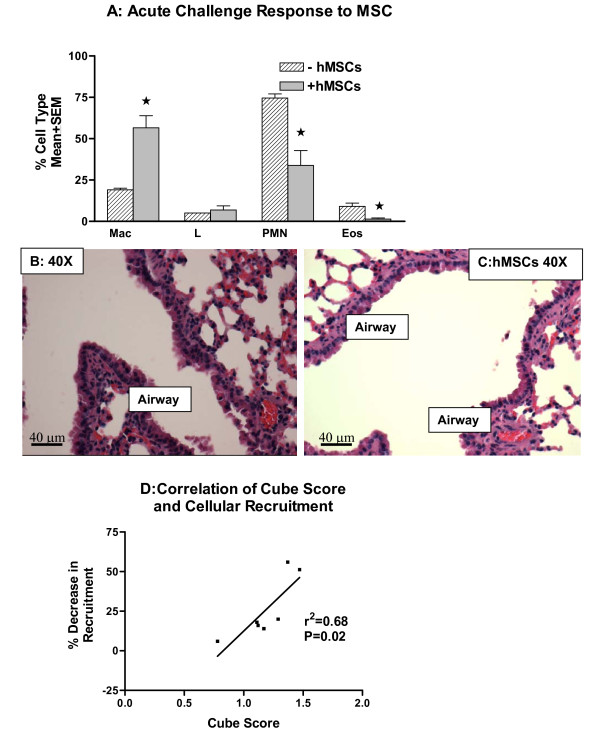
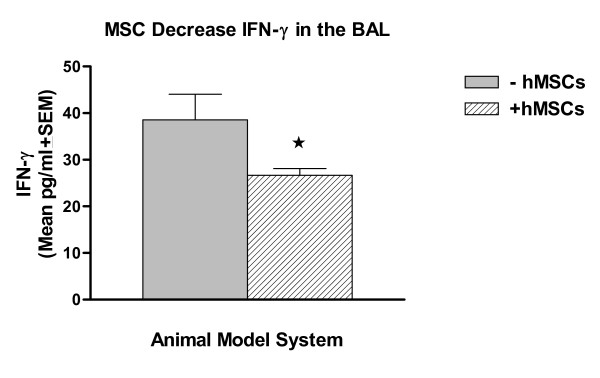
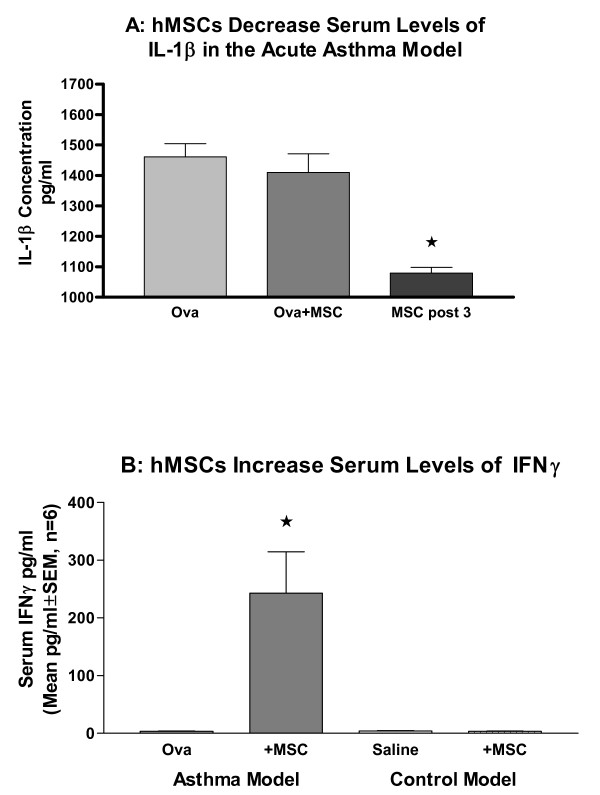
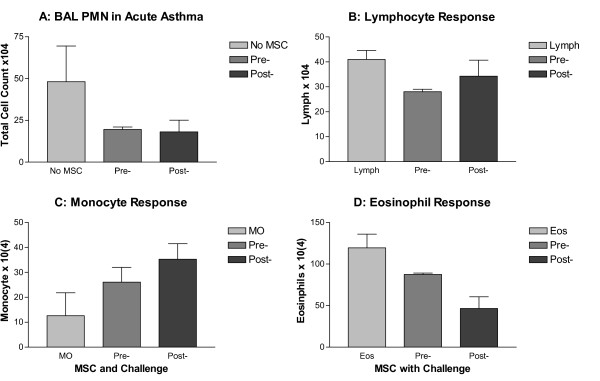
Allogeneic human mesenchymal stem cells (hMSCs) can suppress graft versus host disease (GvHD) and have profound anti-inflammatory and regenerative capacity in stroke, infarct, spinal cord injury, meniscus regeneration, tendinitis, acute renal failure, and heart disease in human and animal models of disease. There is significant clinical hMSC variability in efficacy and the ultimate response in vivo. The challenge in hMSC based therapy is defining the efficacy of hMSC in vivo. Models which may provide insight into hMSC bioactivity in vivo would provide a means to distinguish hMSCs for clinical utility. hMSC function has been described as both regenerative and trophic through the production of bioactive factors. The regenerative component involves the multi-potentiality of hMSC progenitor differentiation. The secreted factors generated by the hMSCs are milieu and injury specific providing unique niches for responses in vivo. These bioactive factors are anti-scarring, angiogenic, anti-apoptotic as well as regenerative. Further, from an immunological standpoint, hMSC's can avoid host immune response, providing xenographic applications. To study the in vivo immuno-regulatory effectiveness of hMSCs, we used the ovalbumin challenge model of acute asthma. This is a quick 3 week in vivo pulmonary inflammation model with readily accessible ways of measuring effectiveness of hMSCs. Our data show that there is a direct correlation between the traditional ceramic cube score to hMSCs attenuation of cellular recruitment due to ovalbumin challenge. The results from these studies verify the in vivo immuno-modulator effectiveness of hMSCs and support the potential use of the ovalbumin model as an in vivo model of hMSC potency and efficacy. Our data also support future directions toward exploring hMSCs as an alternative therapeutic for the treatment of airway inflammation associated with asthma.
Figures
References
-
- Dominici M, Le Blanc K, Mueller I, Slaper-Cortenbach I, Marini F, Krause D, Deans R, Keating A, Prockop D, Horwitz E. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy. 2006;8:315–317. doi: 10.1080/14653240600855905. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
