

Effect of remote ischemic preconditioning on acute kidney injury in nondiabetic patients undergoing coronary artery bypass graft surgery: a secondary analysis of 2 small randomized trials
- PMID: 20974511
- PMCID: PMC2991586
- DOI: 10.1053/j.ajkd.2010.07.014
Effect of remote ischemic preconditioning on acute kidney injury in nondiabetic patients undergoing coronary artery bypass graft surgery: a secondary analysis of 2 small randomized trials
Abstract
Background: Novel treatment strategies are required to reduce the development of acute kidney injury (AKI) in patients undergoing cardiac surgery. In this respect, remote ischemic preconditioning (RIPC), a phenomenon in which transient nonlethal ischemia applied to an organ or tissue protects another organ or tissue from subsequent lethal ischemic injury, is a potential renoprotective strategy.
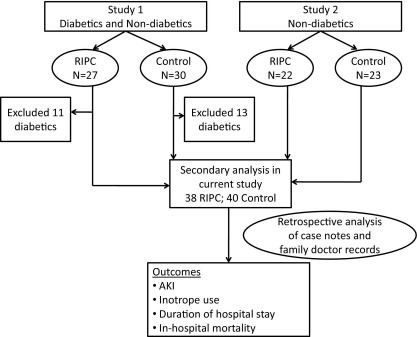
Study design: Secondary analysis of 2 randomized trials.
Setting & participants: 78 consenting selected nondiabetic patients in a university teaching hospital undergoing elective coronary artery bypass graft (CABG) surgery recruited to 2 previously reported randomized studies.
Intervention: RIPC consisted of three 5-minute cycles of right forearm ischemia, induced by inflating a blood pressure cuff on the upper arm to 200 mm Hg, with an intervening 5 minutes of reperfusion, during which time the cuff was deflated. The control consisted of placing an uninflated cuff on the arm for 30 minutes.
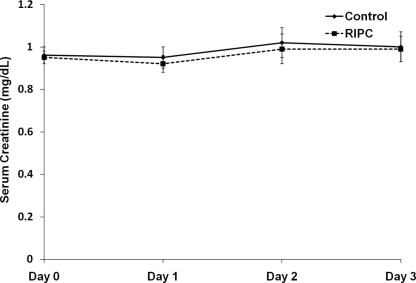
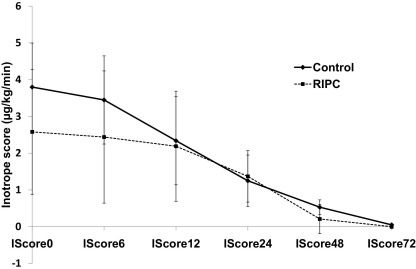
Outcomes: AKI measured using Acute Kidney Injury Network (AKIN) criteria, duration of hospital stay, in-hospital and 30-day mortality.
Results: Numbers of participants with AKI stages 1, 2, and 3 were 1 (3%), 3 (8%), and 0 in the intervention group compared with 10 (25%), 0, and 0 in the control group, respectively (P = 0.005). The decrease in AKI was independent of the effect of concomitant aortic valve replacement and cross-clamp times, which were distributed unevenly between the 2 groups.
Limitations: Retrospective analysis of data. More patients in the RIPC group underwent concomitant aortic valve replacement with CABG; although we have corrected statistically for this imbalance, it remains an important confounding variable.
Conclusions: RIPC induced using transient forearm ischemia decreased the incidence of AKI in nondiabetic patients undergoing elective CABG surgery in this retrospective analysis. A large prospective clinical trial is required to study this effect and clinical outcomes in patients undergoing cardiac surgery.
Copyright © 2010 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Remote ischemic preconditioning: is the groove in the heart?Am J Kidney Dis. 2010 Dec;56(6):1019-22. doi: 10.1053/j.ajkd.2010.09.009. Am J Kidney Dis. 2010. PMID: 21094912 No abstract available.
References
-
- Rosner M.H., Okusa M.D. Acute kidney injury associated with cardiac surgery. Clin J Am Soc Nephrol. 2006;1:19–32. - PubMed
-
- Chertow G.M., Levy E.M., Hammermeister K.E., Grover F., Daley J. Independent association between acute renal failure and mortality following cardiac surgery. Am J Med. 1998;104:343–348. - PubMed
-
- Lassnigg A., Schmidlin D., Mouhieddine M. Minimal changes of serum creatinine predict prognosis in patients after cardiothoracic surgery: a prospective cohort study. J Am Soc Nephrol. 2004;15:1597–1605. - PubMed
-
- Hausenloy D.J., Yellon D.M. Remote ischaemic preconditioning: underlying mechanisms and clinical application. Cardiovasc Res. 2008;79(3):377–386. - PubMed
-
- Walsh S.R., Boyle J.R., Tang T.Y. Remote ischemic preconditioning for renal and cardiac protection during endovascular aneurysm repair: a randomized controlled trial. J Endovasc Ther. 2009;16:680–689. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
