

Efficacy, safety, and tolerability of three regimens for prevention of malaria: a randomized, placebo-controlled trial in Ugandan schoolchildren
- PMID: 20976051
- PMCID: PMC2957410
- DOI: 10.1371/journal.pone.0013438
Efficacy, safety, and tolerability of three regimens for prevention of malaria: a randomized, placebo-controlled trial in Ugandan schoolchildren
Abstract
Background: Intermittent preventive treatment (IPT) is a promising malaria control strategy; however, the optimal regimen remains unclear. We conducted a randomized, single-blinded, placebo-controlled trial to evaluate the efficacy, safety, and tolerability of a single course of sulfadoxine-pyrimethamine (SP), amodiaquine + SP (AQ+SP) or dihydroartemisinin-piperaquine (DP) among schoolchildren to inform IPT.
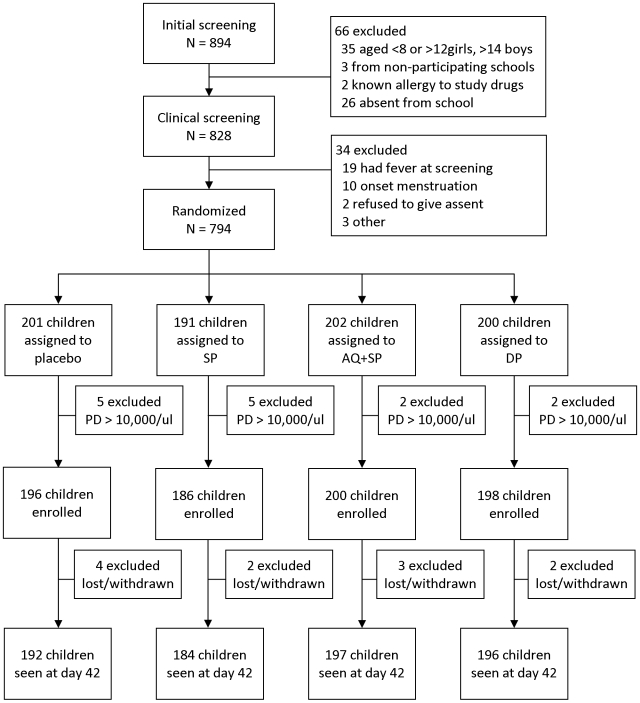
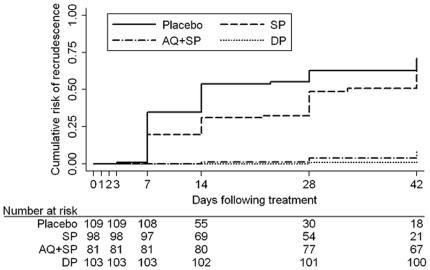
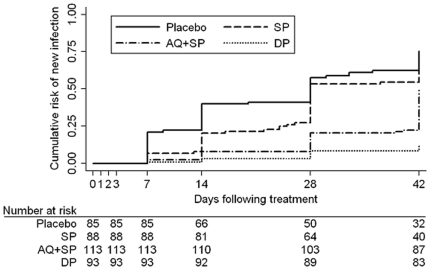
Methods: Asymptomatic girls aged 8 to 12 years and boys aged 8 to 14 years enrolled in two primary schools in Tororo, Uganda were randomized to receive one of the study regimens or placebo, regardless of presence of parasitemia at enrollment, and followed for 42 days. The primary outcome was risk of parasitemia at 42 days. Survival analysis was used to assess differences between regimens.
Results: Of 780 enrolled participants, 769 (98.6%) completed follow-up and were assigned a treatment outcome. The risk of parasitemia at 42 days varied significantly between DP (11.7% [95% confidence interval (CI): 7.9, 17.1]), AQ+SP (44.3% [37.6, 51.5]), and SP (79.7% [95% CI: 73.6, 85.2], p<0.001). The risk of parasitemia in SP-treated children was no different than in those receiving placebo (84.6% [95% CI: 79.1, 89.3], p = 0.22). No serious adverse events occurred, but AQ+SP was associated with increased risk of vomiting compared to placebo (13.0% [95% CI: 9.1, 18.5] vs. 4.7% [95% CI: 2.5, 8.8], respectively, p = 0.003).
Conclusions: DP was the most efficacious and well-tolerated regimen tested, although AQ+SP appears to be a suitable alternative for IPT in schoolchildren. Use of SP for IPT may not be appropriate in areas with high-level SP resistance in Africa.
Trial registration: ClinicalTrials.gov NCT00852371.
Conflict of interest statement
Figures
References
-
- Trape JF, Rogier C, Konate L, Diagne N, Bouganali H, et al. The Dielmo project: a longitudinal study of natural malaria infection and the mechanisms of protective immunity in a community living in a holoendemic area of Senegal. Am J Trop Med Hyg. 1994;51:123–137. - PubMed
-
- Lalloo DG, Olukoya P, Olliaro P. Malaria in adolescence: burden of disease, consequences, and opportunities for intervention. Lancet Infect Dis. 2006;6:780–793. - PubMed
-
- Brooker S. World Bank, Washington DC, USA and Partnership for Child Development, London, UK; 2009. Malaria control in schools: a toolkit on effective education sector responses to malaria in Africa.
