

Population-level reduction in adult mortality after extension of free anti-retroviral therapy provision into rural areas in northern Malawi
- PMID: 20976068
- PMCID: PMC2957442
- DOI: 10.1371/journal.pone.0013499
Population-level reduction in adult mortality after extension of free anti-retroviral therapy provision into rural areas in northern Malawi
Abstract
Background: Four studies from sub-Saharan Africa have found a substantial population-level effect of ART provision on adult mortality. It is important to see if the impact changes with time since the start of treatment scale-up, and as treatment moves to smaller clinics.
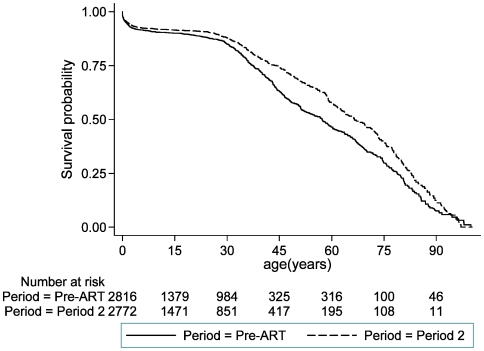
Methods and findings: During 2002-4 a demographic surveillance site (DSS) was established in Karonga district, northern Malawi. Information on births and deaths is collected monthly, with verbal autopsies conducted for all deaths; migrations are updated annually. We analysed mortality trends by comparing three time periods: pre-ART roll-out in the district (August 2002-June 2005), ART period 1 (July 2005-September 2006) when ART was available only in a town 70 km away, and ART period 2 (October 2006-September 2008), when ART was available at a clinic within the DSS area. HIV prevalence and ART uptake were estimated from a sero-survey conducted in 2007/2008. The all-cause mortality rate among 15-59 year olds was 10.2 per 1000 person-years in the pre-ART period (288 deaths/28285 person-years). It fell by 16% in ART period 1 and by 32% in ART period 2 (95% CI 18%-43%), compared with the pre-ART period. The AIDS mortality rate fell from 6.4 to 4.6 to 2.7 per 1000 person-years in the pre-ART period, period 1 and period 2 respectively (rate ratio for period 2 = 0.43, 95% CI 0.33-0.56). There was little change in non-AIDS mortality. Treatment coverage among individuals eligible to start ART was around 70% in 2008.
Conclusions: ART can have a dramatic effect on mortality in a resource-constrained setting in Africa, at least in the early years of treatment provision. Our findings support the decentralised delivery of ART from peripheral health centres with unsophisticated facilities. Continued funding to maintain and further scale-up treatment provision will bring large benefits in terms of saving lives.
Conflict of interest statement
Figures
References
-
- UNAIDS and World Health Organization. Geneva: AIDS epidemic update; 2009.
-
- The Global Fund. Geneva: The Global Fund 2010: Innovation and impact; 2010.
-
- PEPFAR. Making a difference: Funding 2010.
-
- World Health Organization. Geneva: Towards Universal Access: Scaling up priority HIV/AIDS interventions in the health sector: 2009 Progress Report; 2009.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
