

Cost-effectiveness of adolescent pertussis vaccination for the Netherlands: using an individual-based dynamic model
- PMID: 20976213
- PMCID: PMC2955521
- DOI: 10.1371/journal.pone.0013392
Cost-effectiveness of adolescent pertussis vaccination for the Netherlands: using an individual-based dynamic model
Abstract
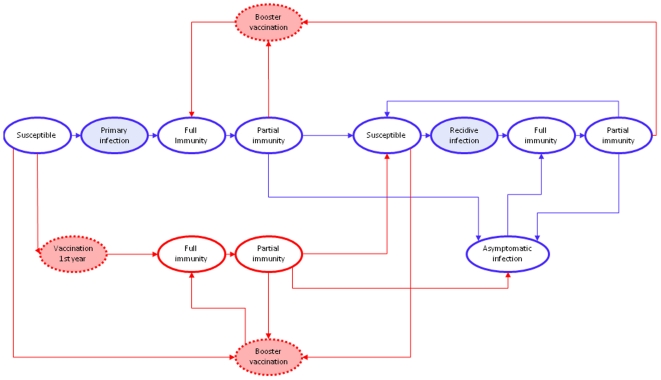
Background: Despite widespread immunization programs, a clear increase in pertussis incidence is apparent in many developed countries during the last decades. Consequently, additional immunization strategies are considered to reduce the burden of disease. The aim of this study is to design an individual-based stochastic dynamic framework to model pertussis transmission in the population in order to predict the epidemiologic and economic consequences of the implementation of universal booster vaccination programs. Using this framework, we estimate the cost-effectiveness of universal adolescent pertussis booster vaccination at the age of 12 years in the Netherlands.
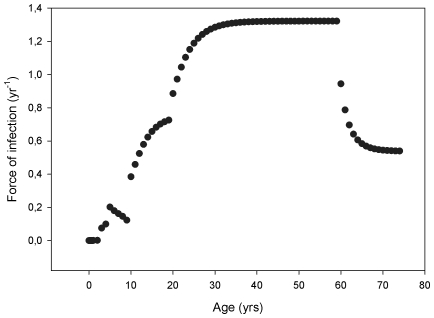
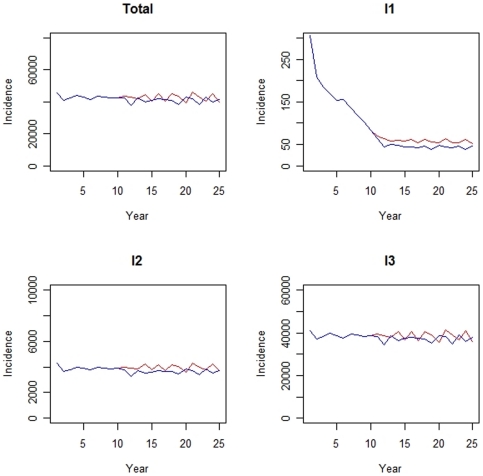
Methods/principal findings: We designed a discrete event simulation (DES) model to predict the epidemiological and economic consequences of implementing universal adolescent booster vaccination. We used national age-specific notification data over the period 1996-2000--corrected for underreporting--to calibrate the model assuming a steady state situation. Subsequently, booster vaccination was introduced. Input parameters of the model were derived from literature, national data sources (e.g. costing data, incidence and hospitalization data) and expert opinions. As there is no consensus on the duration of immunity acquired by natural infection, we considered two scenarios for this duration of protection (i.e. 8 and 15 years). In both scenarios, total pertussis incidence decreased as a result of adolescent vaccination. From a societal perspective, the cost-effectiveness was estimated at €4418/QALY (range: 3205-6364 € per QALY) and €6371/QALY (range: 4139-9549 € per QALY) for the 8- and 15-year protection scenarios, respectively. Sensitivity analyses revealed that the outcomes are most sensitive to the quality of life weights used for pertussis disease.
Conclusions/significance: To our knowledge we designed the first individual-based dynamic framework to model pertussis transmission in the population. This study indicates that adolescent pertussis vaccination is likely to be a cost-effective intervention for The Netherlands. The model is suited to investigate further pertussis booster vaccination strategies.
Conflict of interest statement
Figures
Similar articles
-
Cost-effectiveness of pertussis booster vaccination in the Netherlands.Vaccine. 2012 Nov 26;30(50):7327-31. doi: 10.1016/j.vaccine.2012.06.026. Epub 2012 Jun 27. Vaccine. 2012. PMID: 22749838
-
Cost-effectiveness analysis of a pertussis vaccination programme for Japan considering intergenerational infection.Vaccine. 2013 Jun 12;31(27):2891-7. doi: 10.1016/j.vaccine.2013.03.032. Epub 2013 Apr 6. Vaccine. 2013. PMID: 23570987
-
Pertussis immunization of adolescents in the United States: an economic evaluation.Pediatr Infect Dis J. 2005 May;24(5 Suppl):S75-82. doi: 10.1097/01.inf.0000160918.72953.51. Pediatr Infect Dis J. 2005. PMID: 15876932
-
A critical literature review of health economic evaluations in pertussis booster vaccination.Expert Rev Pharmacoecon Outcomes Res. 2012 Feb;12(1):71-94. doi: 10.1586/erp.11.94. Expert Rev Pharmacoecon Outcomes Res. 2012. PMID: 22280198 Review.
-
Dynamic models for health economic assessments of pertussis vaccines: what goes around comes around...Expert Rev Vaccines. 2012 Dec;11(12):1415-28. doi: 10.1586/erv.12.130. Expert Rev Vaccines. 2012. PMID: 23252386 Review.
Cited by
-
When to use discrete event simulation (DES) for the economic evaluation of health technologies? A review and critique of the costs and benefits of DES.Pharmacoeconomics. 2014 Jun;32(6):547-58. doi: 10.1007/s40273-014-0147-9. Pharmacoeconomics. 2014. PMID: 24627341 Review.
-
Cost-effectiveness of Tdap vaccination of adults aged ≥65 years in the prevention of pertussis in the US: a dynamic model of disease transmission.PLoS One. 2014 Jan 9;9(1):e72723. doi: 10.1371/journal.pone.0072723. eCollection 2014. PLoS One. 2014. PMID: 24416118 Free PMC article.
-
Natural immune boosting in pertussis dynamics and the potential for long-term vaccine failure.Proc Natl Acad Sci U S A. 2011 Apr 26;108(17):7259-64. doi: 10.1073/pnas.1014394108. Epub 2011 Mar 21. Proc Natl Acad Sci U S A. 2011. PMID: 21422281 Free PMC article.
-
Reduced-antigen, combined diphtheria, tetanus and acellular pertussis vaccine, adsorbed (Boostrix®): a review of its properties and use as a single-dose booster immunization.Drugs. 2012 Sep 10;72(13):1765-91. doi: 10.2165/11209630-000000000-00000. Drugs. 2012. PMID: 22931522 Review.
-
Burden of Pertussis in Individuals with a Diagnosis of Asthma: A Retrospective Database Study in England.J Asthma Allergy. 2022 Jan 11;15:35-51. doi: 10.2147/JAA.S335960. eCollection 2022. J Asthma Allergy. 2022. PMID: 35046668 Free PMC article.
References
-
- Tan T, Trindade E, Skowronski D. Epidemiology of Pertussis. Pediatr Infect Dis J. 2005;24:S10–18. - PubMed
-
- Neppelenbroek SE, De Melker HE, Schellekens JFP, Conyn-van Spaendonck MAE. The incidence of pertussis in the Netherlands remains high since an outbreak occurred in 1996. Euro Surveill. 1999;4:133–134. - PubMed
-
- Schellekens JFP, Wirsing von König CH, Gardner P. Pertussis sources of infection and routes of transmission in the vaccination era. Pediatr Infect Dis J. 2005;24:S19–24. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
