

Quantitative structural MRI for early detection of Alzheimer's disease
- PMID: 20977326
- PMCID: PMC3182103
- DOI: 10.1586/ern.10.162
Quantitative structural MRI for early detection of Alzheimer's disease
Abstract
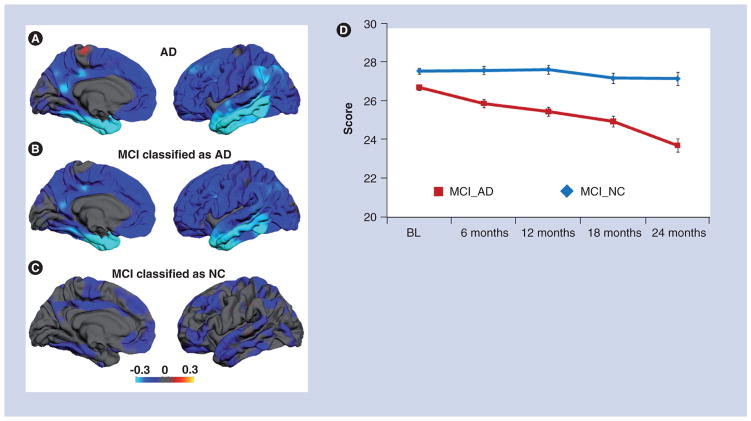
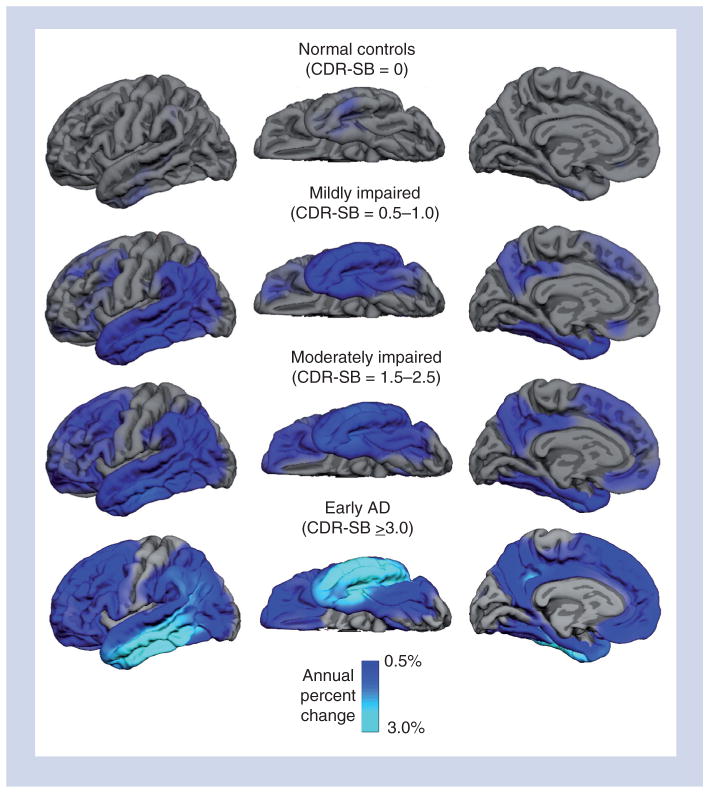
Alzheimer's disease (AD) is a common progressive neurodegenerative disorder that is not currently diagnosed until a patient reaches the stage of dementia. There is a pressing need to identify AD at an earlier stage, so that treatment, when available, can begin early. Quantitative structural MRI is sensitive to the neurodegeneration that occurs in mild and preclinical AD, and is predictive of decline to dementia in individuals with mild cognitive impairment. Objective evidence of ongoing brain atrophy will be critical for risk/benefit decisions once potentially aggressive, disease-modifying treatments become available. Recent advances have paved the way for the use of quantitative structural MRI in clinical practice, and initial clinical use has been promising. However, further experience with these measures in the relatively unselected patient populations seen in clinical practice is needed to complete translation of the recent enormous advances in scientific knowledge of AD into the clinical realm.
Figures
References
Website
-
- Alzheimer’s Association: Recommendations to Update Diagnostic Criteria. www.alz.org/research/diagnostic_criteria.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical