

Endovascular treatment of intracranial aneurysms associated with moyamoya disease or moyamoya syndrome
- PMID: 20977854
- PMCID: PMC3277993
- DOI: 10.1177/159101991001600302
Endovascular treatment of intracranial aneurysms associated with moyamoya disease or moyamoya syndrome
Abstract
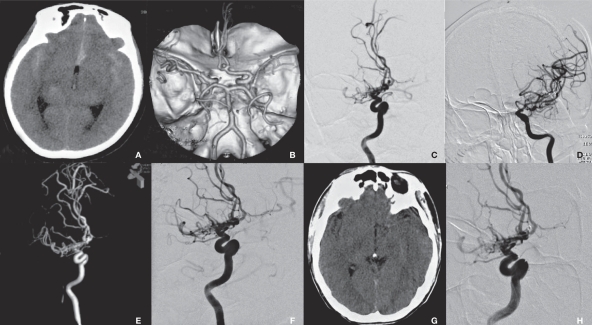
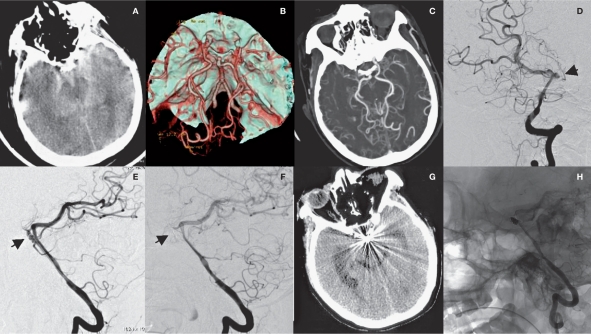
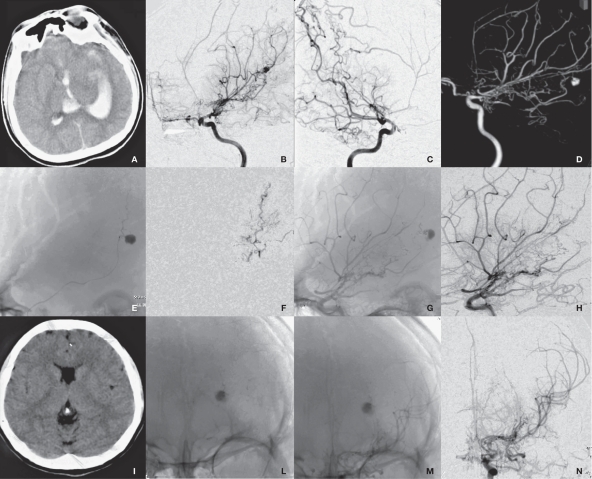
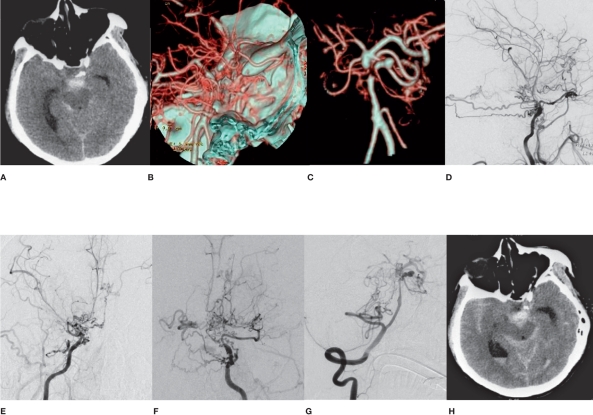
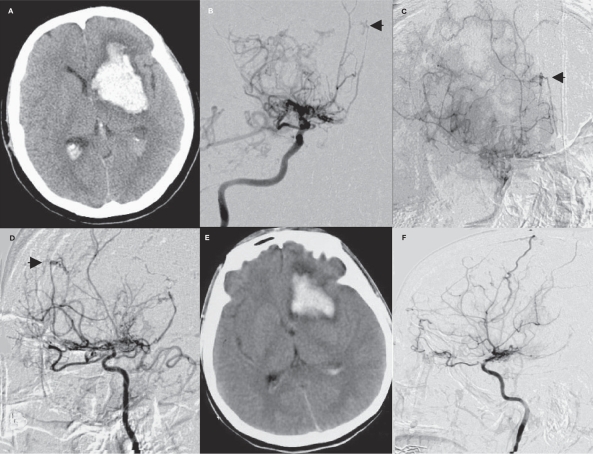
Direct surgical clipping proves to be difficult and dangerous for intracranial aneurysms associated with moyamoya disease (MMD) or moyamoya syndrome (MMS). This study presents our clinical experience of endovascular embolization of intracranial aneurysms associated with these diseases. A total of 13 cases of intracranial aneurysms associated with MMD or MMS were treated by endovascular embolization between January 2001 and January 2009. Patients were divided into two groups: a saccular aneurysm group (n=10) and a pseudoaneurysm group (n=3). Different endovascular therapeutic strategies were employed for each type of case. Of the 13 cases, 11 received successful endovascular embolization and had an uneventful postoperative course during one to two years of follow-up. However, endovascular embolization failed in the other two cases, of whom one died from rebleeding after the five-month follow-up, while the other was conservatively treated and experienced no rebleeding during the two-year follow-up. A favorable prognosis may be secured through careful selection of endovascular treatment regimens for patients with intracranial aneurysms associated with MMD or MMS according to the site of intracranial aneurysms.
Figures
References
-
- Nishimoto A. Moyamoya disease (author's transl) Neurol Med Chir (Tokyo) 1979;19(3):221–228. - PubMed
-
- Kelly ME, Bell-Stephens TE, Marks MP, et al. Progression of unilateral moyamoya disease: A clinical series. Cerebrovasc Dis. 2006;22(2-3):109–15. - PubMed
-
- Natori Y, Ikezaki K, Matsushima T, et al. ‘Angiographic moyamoya’ its definition, classification, and therapy. Clin Neurol Neurosurg. 1997;99(Suppl 2):S168–72. - PubMed
-
- Kawaguchi S, Sakaki T, Kakizaki T, et al. Clinical features of the haemorrhage type moyamoya disease based on 31 cases. Acta Neurochir (Wien) 1996;138(10):1200–10. - PubMed
-
- Iwama T, Todaka T, Hashimoto N. Direct surgery for major artery aneurysm associated with Moyamoya disease. Clin Neurol Neurosurg. 1997;99:191–193. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
