

Glycated hemoglobin and the risk of kidney disease and retinopathy in adults with and without diabetes
- PMID: 20978092
- PMCID: PMC3012185
- DOI: 10.2337/db10-1198
Glycated hemoglobin and the risk of kidney disease and retinopathy in adults with and without diabetes
Abstract
Objective: Glycated hemoglobin was recently recommended for use as a diagnostic test for diabetes. We examined the association between 2010 American Diabetes Association diagnostic cut points for glycated hemoglobin and microvascular outcomes (chronic kidney disease, end-stage renal disease [ESRD], and retinopathy) and formally tested for the presence of risk thresholds in the relationships of glycated hemoglobin with these outcomes.
Research design and methods: Prospective cohort and cross-sectional analyses of 11,357 participants (773 with a history of diagnosed diabetes) from the Atherosclerosis Risk in Communities (ARIC) Study.
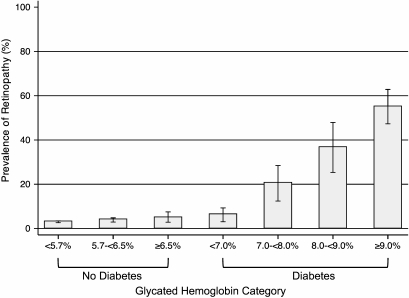
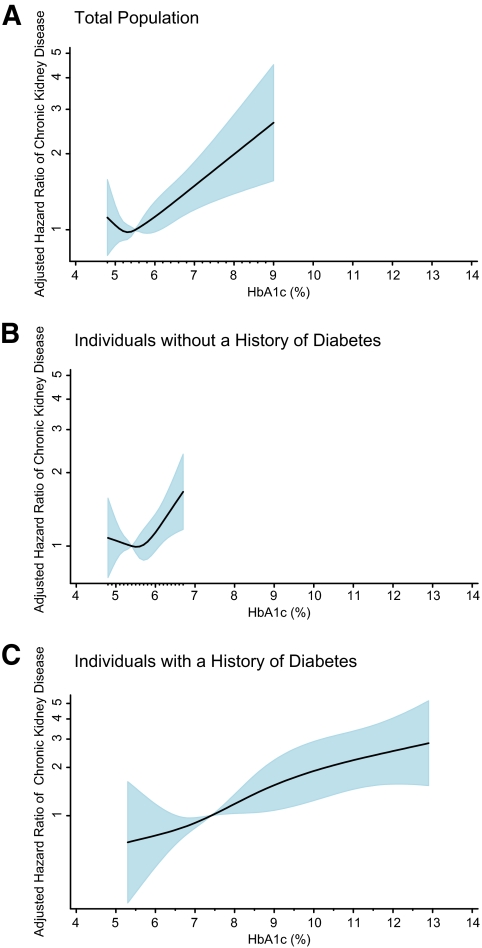
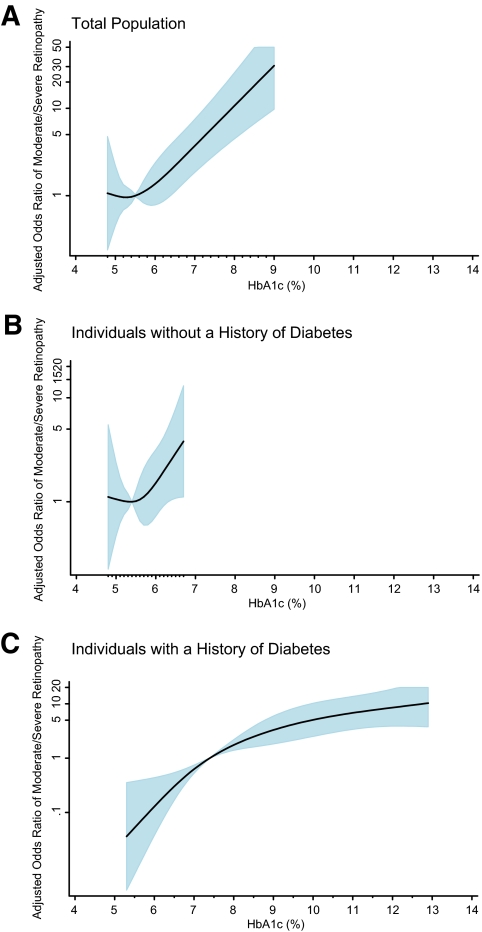
Results: During a median of 14 years of follow-up of individuals without diagnosed diabetes at baseline, clinical categories of glycated hemoglobin were associated with risk of chronic kidney disease, with adjusted hazard ratios (HRs) of 1.12 (0.94-1.34) and 1.39 (1.04-1.85) for glycated hemoglobin 5.7-6.4% and ≥6.5%, respectively, as compared with <5.7% (P trend = 0.002). The corresponding HRs for ESRD were 1.51 (0.82-2.76) and 1.98 (0.83-4.73), respectively (P trend = 0.047). In the absence of diagnosed diabetes, glycated hemoglobin was cross sectionally associated with the presence of moderate/severe retinopathy, with adjusted odds ratios of 1.42 (0.69-2.92) and 2.91 (1.19-7.11) for glycated hemoglobin 5.7-<6.5% and ≥6.5%, respectively, compared with <5.7% (P trend = 0.011). Risk associations were stronger among individuals with a history of diabetes. We did not observe significant thresholds in the associations of glycated hemoglobin with kidney disease risk or retinopathy.
Conclusions: These data from a community-based, biracial population support the use of new 2010 American Diabetes Association glycated hemoglobin cut points for the diagnosis of diabetes.
Figures
References
-
- Klein R, Klein BE, Moss SE, Davis MD, DeMets DL: Glycosylated hemoglobin predicts the incidence and progression of diabetic retinopathy. JAMA 1988;260:2864–2871 - PubMed
-
- Davidson MB, Schriger DL, Peters AL, Lorber B: Relationship between fasting plasma glucose and glycosylated hemoglobin: potential for false-positive diagnoses of type 2 diabetes using new diagnostic criteria. JAMA 1999;281:1203–1210 - PubMed
-
- Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 1997;20:1183–1197 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01 HC055016/HL/NHLBI NIH HHS/United States
- N01 HC055019/HL/NHLBI NIH HHS/United States
- N01-HC-55016/HC/NHLBI NIH HHS/United States
- P30 DK079637/DK/NIDDK NIH HHS/United States
- N01-HC-55021/HC/NHLBI NIH HHS/United States
- N01-HC-55019/HC/NHLBI NIH HHS/United States
- T32 HL-007024/HL/NHLBI NIH HHS/United States
- P60 DK079637/DK/NIDDK NIH HHS/United States
- N01-HC-55020/HC/NHLBI NIH HHS/United States
- R01 DK076770/DK/NIDDK NIH HHS/United States
- N01 HC055018/HL/NHLBI NIH HHS/United States
- N01 HC055022/HL/NHLBI NIH HHS/United States
- N01-HC-55018/HC/NHLBI NIH HHS/United States
- K24 DK062222/DK/NIDDK NIH HHS/United States
- R01 DK-076770/DK/NIDDK NIH HHS/United States
- R21 DK-080294/DK/NIDDK NIH HHS/United States
- P60 DK-079637/DK/NIDDK NIH HHS/United States
- N01-HC-55022/HC/NHLBI NIH HHS/United States
- N01 HC055021/HL/NHLBI NIH HHS/United States
- T32 HL007024/HL/NHLBI NIH HHS/United States
- N01 HC055015/HL/NHLBI NIH HHS/United States
- N01 HC055020/HL/NHLBI NIH HHS/United States
- K01 DK076595/DK/NIDDK NIH HHS/United States
- N01-HC-55015/HC/NHLBI NIH HHS/United States
- K01 DK-076595/DK/NIDDK NIH HHS/United States
- K24 DK-62222/DK/NIDDK NIH HHS/United States
- R21 DK080294/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
