

Glycemic thresholds for diabetes-specific retinopathy: implications for diagnostic criteria for diabetes
- PMID: 20978099
- PMCID: PMC3005450
- DOI: 10.2337/dc10-1206
Glycemic thresholds for diabetes-specific retinopathy: implications for diagnostic criteria for diabetes
Erratum in
- Diabetes Care. 2011 Aug;34(8):1888
Abstract
Objective: To re-evaluate the relationship between glycemia and diabetic retinopathy.
Research design and methods: We conducted a data-pooling analysis of nine studies from five countries with 44,623 participants aged 20-79 years with gradable retinal photographs. The relationship between diabetes-specific retinopathy (defined as moderate or more severe retinopathy) and three glycemic measures (fasting plasma glucose [FPG; n = 41,411], 2-h post oral glucose load plasma glucose [2-h PG; n = 21,334], and A1C [n = 28,010]) was examined.
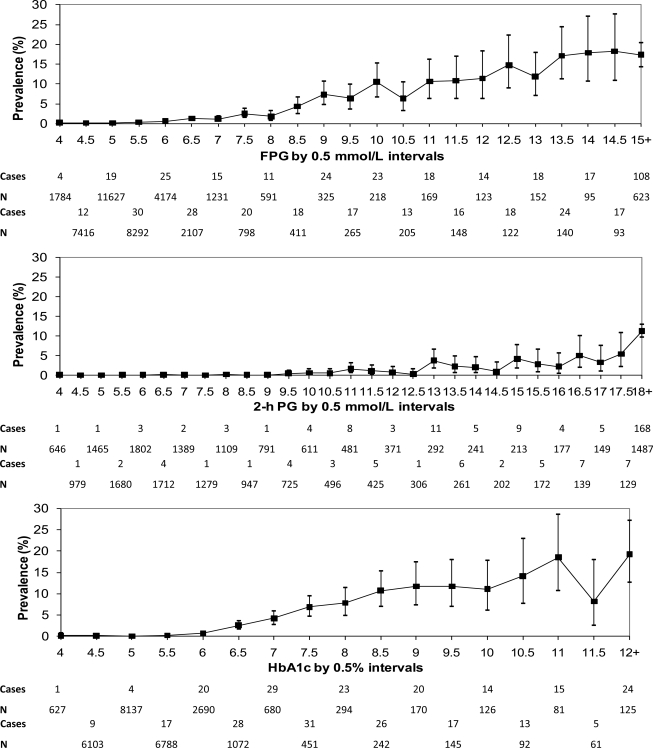
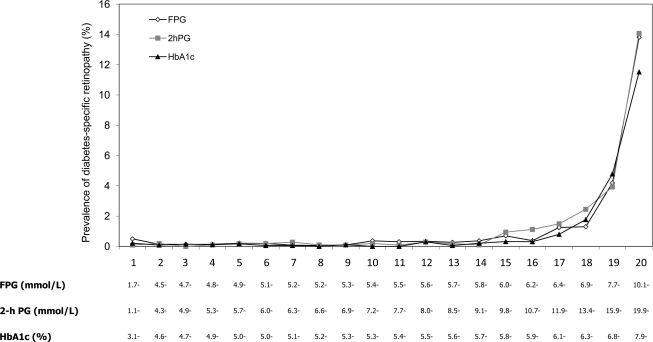
Results: When diabetes-specific retinopathy was plotted against continuous glycemic measures, a curvilinear relationship was observed for FPG and A1C. Diabetes-specific retinopathy prevalence was low for FPG <6.0 mmol/l and A1C <6.0% but increased above these levels. Based on vigintile (20 groups with equal numbers) distributions, glycemic thresholds for diabetes-specific retinopathy were observed over the range of 6.4-6.8 mmol/l for FPG, 9.8-10.6 mmol/l for 2-h PG, and 6.3-6.7% for A1C. Thresholds for diabetes-specific retinopathy from receiver-operating characteristic curve analyses were 6.6 mmol/l for FPG, 13.0 mmol/l for 2-h PG, and 6.4% for A1C.
Conclusions: This study broadens the evidence based on diabetes diagnostic criteria. A narrow threshold range for diabetes-specific retinopathy was identified for FPG and A1C but not for 2-h PG. The combined analyses suggest that the current diabetes diagnostic level for FPG could be lowered to 6.5 mmol/l and that an A1C of 6.5% is a suitable alternative diagnostic criterion.
Figures
References
-
- World Health Organization and International Diabetes Federation Definition and diagnosis of diabetes mellitus and intermediate hyperglycemia: report of a WHO/IDF consultation. World Health Organization: Geneva, 2006
-
- The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus Report of the expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care 1997;20:1183–1197 - PubMed
-
- Ito C, Maeda R, Ishida S, Harada H, Inoue N, Sasaki H: Importance of OGTT for diagnosing diabetes mellitus based on prevalence and incidence of retinopathy. Diabetes Res Clin Pract 2000;49:181–186 - PubMed
-
- Tapp RJ, Zimmer PZ, Harper CA, de Courten MP, McCarty DJ, Balkau B, Taylor HR, Welbourn TA, Shaw JE: AusDiab Study Group Diagnostic thresholds for diabetes: the association of retinopathy and albuminuria with glycaemia. Diabetes Res Clin Pract 2006;73:315–321 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01 HC055016/HL/NHLBI NIH HHS/United States
- N01 HC055019/HL/NHLBI NIH HHS/United States
- N01-HC-55016/HC/NHLBI NIH HHS/United States
- N01 HC055015/HL/NHLBI NIH HHS/United States
- N01-HC-55021/HC/NHLBI NIH HHS/United States
- N01 HC055020/HL/NHLBI NIH HHS/United States
- N01-HC-55019/HC/NHLBI NIH HHS/United States
- N01-HC-55015/HC/NHLBI NIH HHS/United States
- N01-HC-55020/HC/NHLBI NIH HHS/United States
- ImNIH/Intramural NIH HHS/United States
- N01 HC055018/HL/NHLBI NIH HHS/United States
- N01 HC055022/HL/NHLBI NIH HHS/United States
- N01-HC-55018/HC/NHLBI NIH HHS/United States
- N01-HC-55022/HC/NHLBI NIH HHS/United States
- N01 HC055021/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
