

Lenalidomide in nonmetastatic biochemically relapsed prostate cancer: results of a phase I/II double-blinded, randomized study
- PMID: 20978144
- PMCID: PMC3444815
- DOI: 10.1158/1078-0432.CCR-10-1928
Lenalidomide in nonmetastatic biochemically relapsed prostate cancer: results of a phase I/II double-blinded, randomized study
Abstract
Purpose: To evaluate the safety and activity of 6 months of treatment with lenalidomide at 5 or 25 mg/d in nonmetastatic biochemically relapsed prostate cancer.
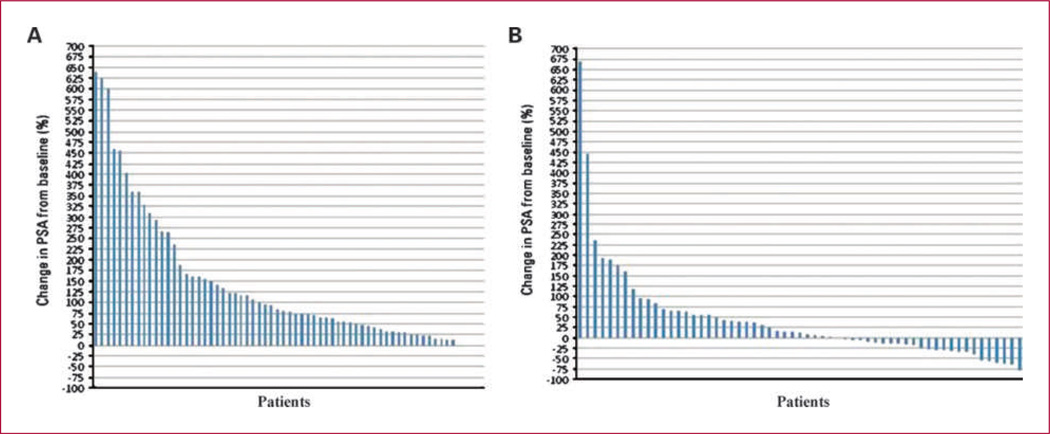
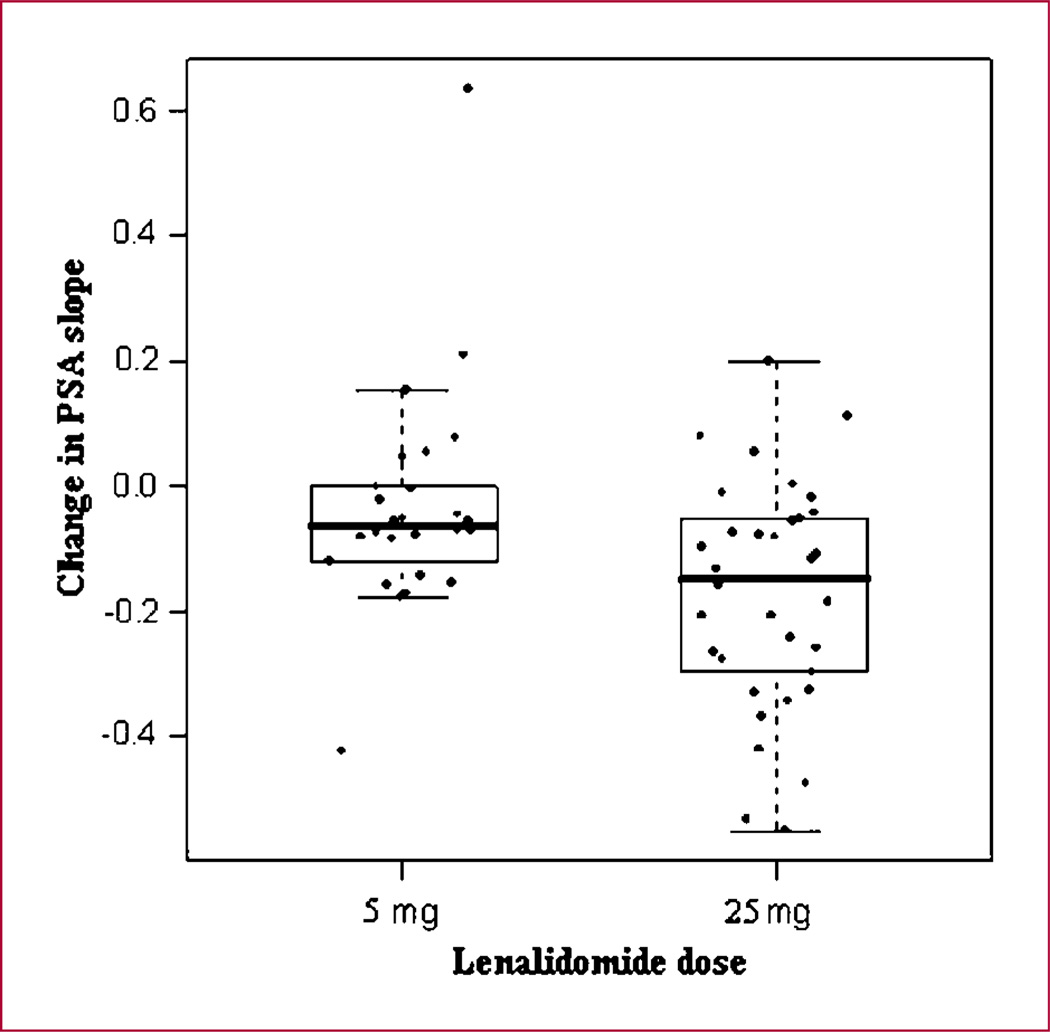
Experimental design: Sixty men with non-castrate, nonmetastatic, biochemically relapsed prostate cancer were stratified by prostate-specific antigen (PSA) doubling time, surgery/radiation therapy, prior androgen deprivation therapy (ADT), and randomized to lenalidomide 5 mg (n = 26) or 25 mg/d (n = 34) for 3 weeks repeated monthly for 6 months or until dose-limiting toxicity or disease progression. Toxicity was evaluated monthly, and PSAs and X-rays/scans every 6 months. Study size was determined to detect a progression rate of 40% at 6 months in either arm with 85% power (compared with a rate of 80% in the population receiving no treatment). Changes in PSA slopes were calculated using the regression of the log PSA for each patient before and during the initial 6 months and compared by t test.
Results: Baseline variables were balanced between arms. Grade 3/4 toxicity rates were 12% (n = 3) with 5 mg and 29% (n = 10) with 25 mg (P = 0.1), most commonly neutropenia (five patients, all on 25 mg). Two patients per arm had thromboembolic events. The change in PSA slope was greater with 25 mg versus 5 mg [-0.172 (-0.24 to -0.11) versus -0.033 (-0.11 to 0.04); P = 0.005]. With a mean follow-up of 31.4 months (range 14-44), five patients on 25 mg and one patient on 5 mg remain on the study.
Conclusions: Lenalidomide has acceptable toxicity and is associated with long-term disease stabilization and PSA declines. Randomized studies evaluating conventional clinical disease end points in this patient population are planned.
©2010 AACR.
Conflict of interest statement
No potential conflicts of interest were disclosed.
Figures
References
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin. 2010;60:277–300. [Epub ahead of print]. - PubMed
-
- Keating NL, O'Malley AJ, Smith MR. Diabetes and cardiovascular disease during androgen deprivation therapy for prostate cancer. J Clin Oncol. 2006;24:4448–4456. - PubMed
-
- Moul JW, Bañez LL, Freedland SJ. Rising PSA in nonmetastatic prostate cancer. Oncology (Williston Park) 2007;21:1436–1445. (Review). - PubMed
-
- Pound C, Partin A, Eisenberger M, Chan DW, Pearson JD, Walsh PC. Natural history of progression after PSA elevation following radical prostatectomy. JAMA. 1999;281:1591–1597. - PubMed
-
- Zelefsky MJ, Ben-Porat L, Scher HI, et al. Outcome predictors for the increasing PSA state after definitive external-beam radiotherapy for prostate cancer. J Clin Oncol. 2005;23:826–831. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
