

Coagulation abnormalities in the trauma patient: the role of point-of-care thromboelastography
- PMID: 20978993
- PMCID: PMC4369086
- DOI: 10.1055/s-0030-1265289
Coagulation abnormalities in the trauma patient: the role of point-of-care thromboelastography
Abstract
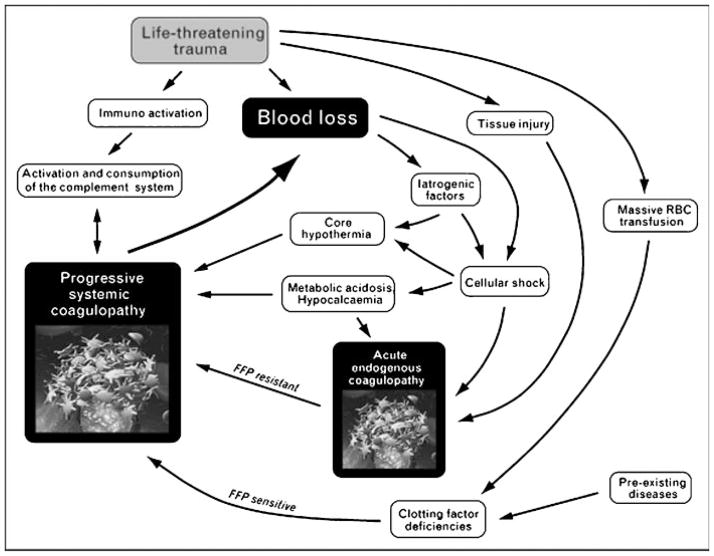
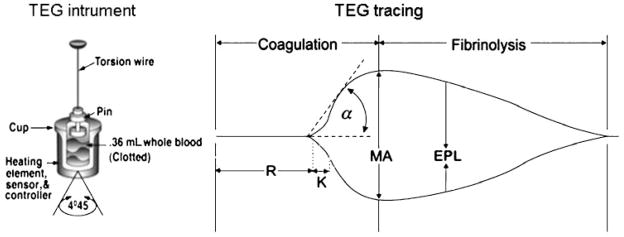
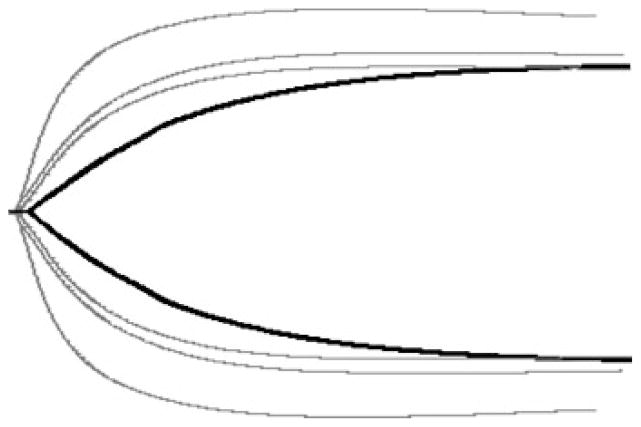
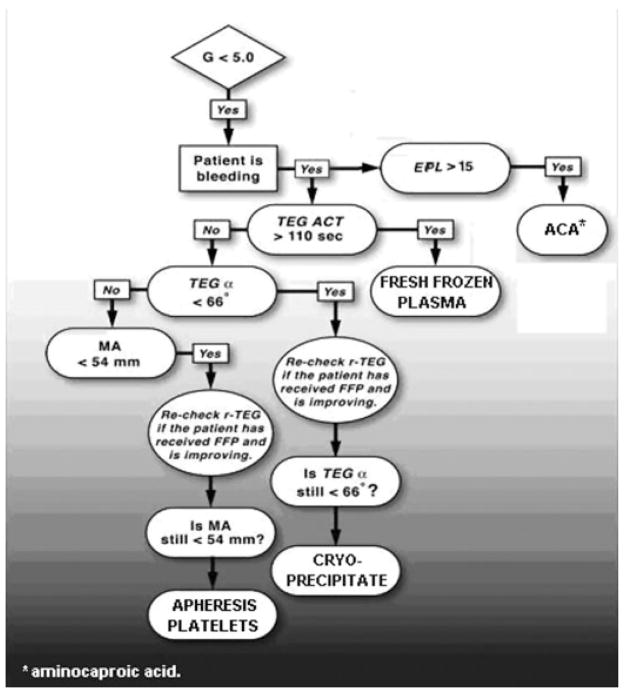
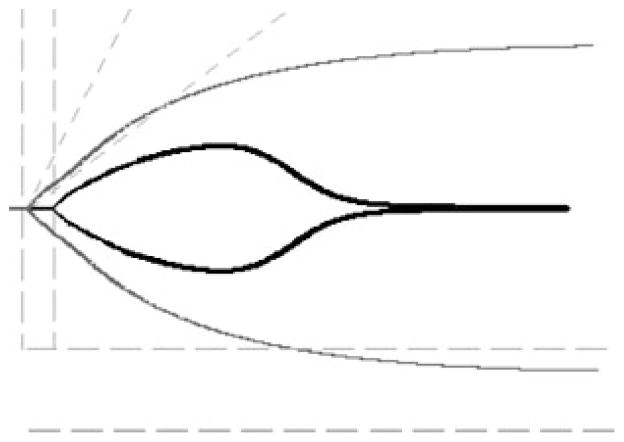
Current recommendations for resuscitation of the critically injured patient are limited by a lack of point-of-care (POC) assessment of coagulation status. Accordingly, the potential exists for indiscriminant blood component administration. Furthermore, although thromboembolic events have been described shortly after injury, the time sequence of post-injury coagulation changes is unknown. Our current understanding of hemostasis has shifted from a classic view, in which coagulation was considered a chain of catalytic enzyme reactions, to the cell-based model (CBM), representing the interplay between the cellular and plasma components of clot formation. Thromboelastography (TEG), a time-sensitive dynamic assay of the viscoelastic properties of blood, closely parallels the CBM, permitting timely, goal-directed restoration of hemostasis via POC monitoring of coagulation status. TEG-based therapy allows for goal-directed blood product administration in trauma, with potential avoidance of the complications resulting from overzealous component administration, as well as the ability to monitor post-injury coagulation status and thromboprophylaxis. This overview addresses coagulation status and thromboprophylaxis management in the trauma patient and the emerging role of POC TEG.
© Thieme Medical Publishers.
Figures
References
-
- Sauaia A, Moore FA, Moore EE, et al. Epidemiology of trauma deaths: a reassessment. J Trauma. 1995;38:185–193. - PubMed
-
- Kauvar DS, Lefering R, Wade CE. Impact of hemorrhage on trauma outcome: an overview of epidemiology, clinical presentations, and therapeutic considerations. J Trauma. 2006;60(6, Suppl):S3–S11. - PubMed
-
- Cosgriff N, Moore EE, Sauaia A, Kenny-Moynihan M, Burch JM, Galloway B. Predicting life-threatening coagulopathy in the massively transfused trauma patient: hypothermia and acidoses revisited. J Trauma. 1997;42(5):857–861. discussion 861–862. - PubMed
-
- MacLeod JB, Lynn M, McKenney MG, Cohn SM, Murtha M. Early coagulopathy predicts mortality in trauma. J Trauma. 2003;55(1):39–44. - PubMed
-
- Kashuk JL, Moore EE, Millikan JS, Moore JB. Major abdominal vascular trauma—a unified approach. J Trauma. 1982;22(8):672–679. - PubMed
