

Tiotropium bromide step-up therapy for adults with uncontrolled asthma
- PMID: 20979471
- PMCID: PMC3011177
- DOI: 10.1056/NEJMoa1008770
Tiotropium bromide step-up therapy for adults with uncontrolled asthma
Abstract
Background: Long-acting beta-agonist (LABA) therapy improves symptoms in patients whose asthma is poorly controlled by an inhaled glucocorticoid alone. Alternative treatments for adults with uncontrolled asthma are needed.
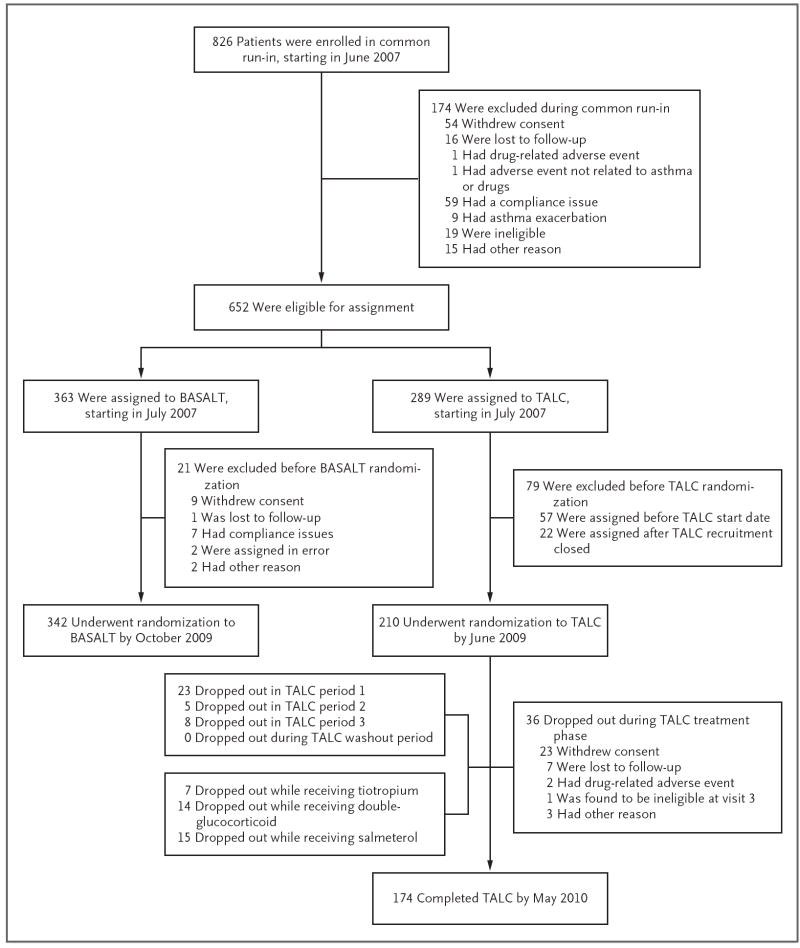
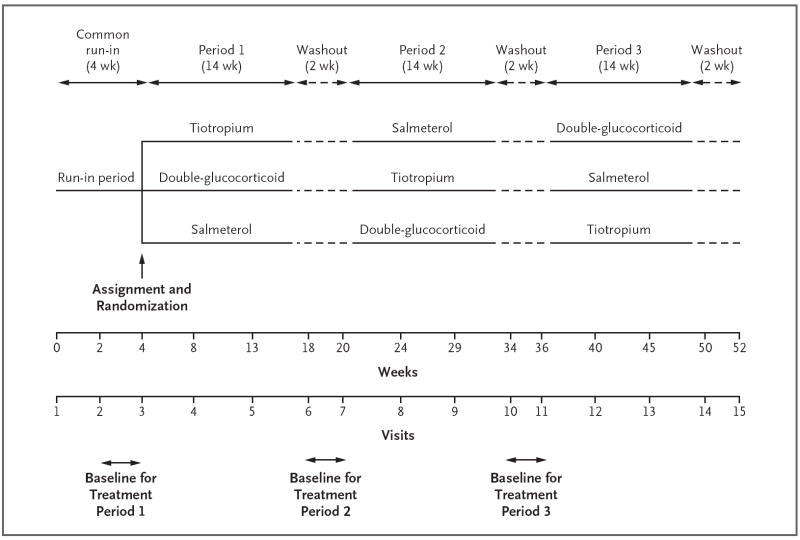
Methods: In a three-way, double-blind, triple-dummy crossover trial involving 210 patients with asthma, we evaluated the addition of tiotropium bromide (a long-acting anticholinergic agent approved for the treatment of chronic obstructive pulmonary disease but not asthma) to an inhaled glucocorticoid, as compared with a doubling of the dose of the inhaled glucocorticoid (primary superiority comparison) or the addition of the LABA salmeterol (secondary noninferiority comparison).
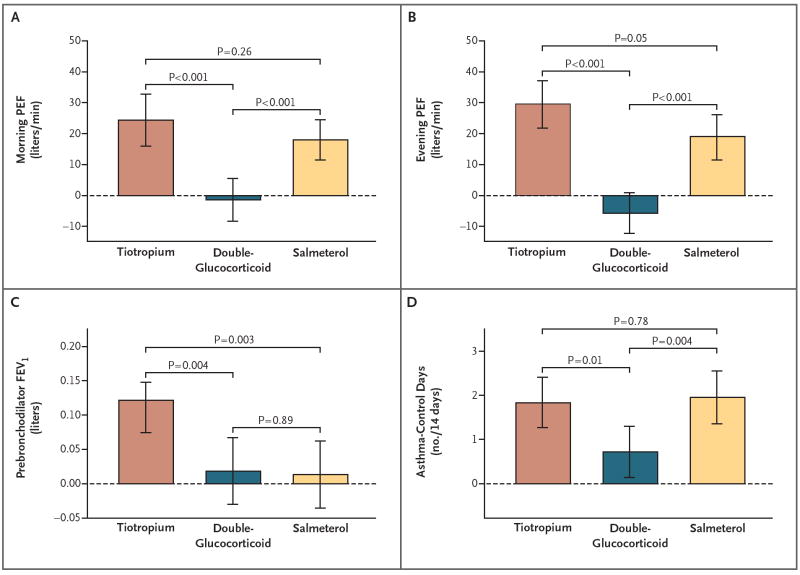
Results: The use of tiotropium resulted in a superior primary outcome, as compared with a doubling of the dose of an inhaled glucocorticoid, as assessed by measuring the morning peak expiratory flow (PEF), with a mean difference of 25.8 liters per minute (P<0.001) and superiority in most secondary outcomes, including evening PEF, with a difference of 35.3 liters per minute (P<0.001); the proportion of asthma-control days, with a difference of 0.079 (P=0.01); the forced expiratory volume in 1 second (FEV1) before bronchodilation, with a difference of 0.10 liters (P=0.004); and daily symptom scores, with a difference of -0.11 points (P<0.001). The addition of tiotropium was also noninferior to the addition of salmeterol for all assessed outcomes and increased the prebronchodilator FEV1 more than did salmeterol, with a difference of 0.11 liters (P=0.003).
Conclusions: When added to an inhaled glucocorticoid, tiotropium improved symptoms and lung function in patients with inadequately controlled asthma. Its effects appeared to be equivalent to those with the addition of salmeterol. (Funded by the National Heart, Lung, and Blood Institute; ClinicalTrials.gov number, NCT00565266.).
Figures
Comment in
-
Products at risk.N Engl J Med. 2010 Oct 28;363(18):1763. doi: 10.1056/NEJMe1010348. Epub 2010 Sep 19. N Engl J Med. 2010. PMID: 20979478 No abstract available.
-
Anticholinergics for patients with asthma?N Engl J Med. 2010 Oct 28;363(18):1764-5. doi: 10.1056/NEJMe1009429. Epub 2010 Sep 19. N Engl J Med. 2010. PMID: 20979479 No abstract available.
-
Tiotropium bromide in asthma patients: an alternative to inhaled long-acting beta-agonists?J R Coll Physicians Edinb. 2010 Dec;40(4):321-2. doi: 10.4997/JRCPE.2010.425. J R Coll Physicians Edinb. 2010. PMID: 21132141 No abstract available.
-
Tiotropium step-up therapy in asthma.N Engl J Med. 2011 Feb 10;364(6):578; author reply 578-9. doi: 10.1056/NEJMc1013636. N Engl J Med. 2011. PMID: 21306255 No abstract available.
-
Tiotropium step-up therapy in asthma.N Engl J Med. 2011 Feb 10;364(6):578; author reply 578-9. doi: 10.1056/NEJMc1013636. N Engl J Med. 2011. PMID: 21306256 No abstract available.
-
ACP Journal Club. Tiotropium plus beclomethasone was more effective than doubling beclomethasone for asthma.Ann Intern Med. 2011 Feb 15;154(4):JC2-4. doi: 10.7326/0003-4819-154-4-201102150-02004. Ann Intern Med. 2011. PMID: 21320931 No abstract available.
-
Recommended reading from the duke university pulmonary critical care fellowship training program: loretta g. Que, program director.Am J Respir Crit Care Med. 2011 Oct 15;184(8):980-1. doi: 10.1164/rccm.201104-0763RR. Am J Respir Crit Care Med. 2011. PMID: 22003149 No abstract available.
References
-
- Global Initiative for Asthma (GINA) home page. http://www.ginasthma.com.
-
- Bethesda, MD: National Heart, Lung, and Blood Institute; 2007. National Asthma Education and Prevention Program. Expert panel report III: guidelines for the diagnosis and management of asthma. (NIH publication no. 08-4051). http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm.
-
- Woolcock A, Lundback B, Ringdal N, Jacques LA. Comparison of addition of salmeterol to inhaled steroids with doubling of the dose of inhaled steroids. Am J Respir Crit Care Med. 1996;153:1481–8. - PubMed
-
- Gibson PG, Powell H, Ducharme FM. Differential effects of maintenance long-acting beta-agonist and inhaled corticosteroid on asthma control and asthma exacerbations. J Allergy Clin Immunol. 2007;119:344–50. - PubMed
-
- Rockville, MD: Food and Drug Administration; Long-acting beta agonist (LABA) information. http://www.fda.gov/Drugs/DrugSafety/InformationbyDrugClass/ucm199565.htm.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical