

Elasticity-based determination of isovolumetric phases in the human heart
- PMID: 20979648
- PMCID: PMC2987769
- DOI: 10.1186/1532-429X-12-60
Elasticity-based determination of isovolumetric phases in the human heart
Abstract
BACKGROUND/MOTIVATION: To directly determine isovolumetric cardiac time intervals by magnetic resonance elastography (MRE) using the magnitude of the complex signal for deducing morphological information combined with the phase of the complex signal for tension-relaxation measurements.
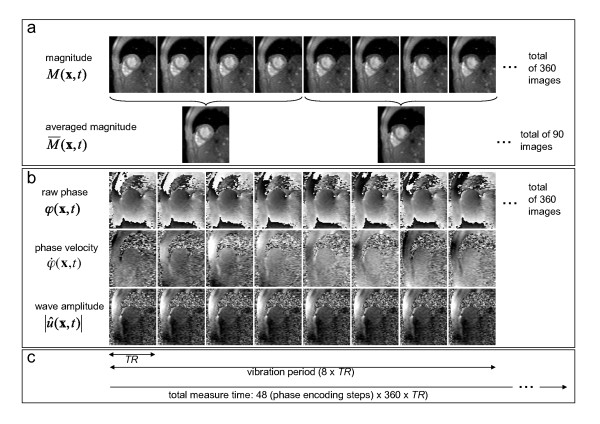
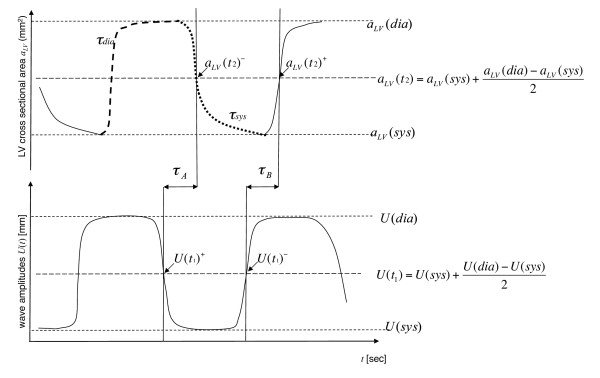
Methods: Thirty-five healthy volunteers and 11 patients with relaxation abnormalities were subjected to transthoracic wave stimulation using vibrations of approximately 25 Hz. A k-space-segmented, ECG-gated gradient-recalled echo steady-state sequence with a 500-Hz bipolar motion-encoding gradient was used for acquiring a series of 360 complex images of a short-axis view of the heart at a frame rate of less than 5.2 ms. Magnitude images were employed for measuring the cross-sectional area of the left ventricle, while phase images were used for analyzing the amplitudes of the externally induced waves. The delay between the decrease in amplitude and onset of ventricular contraction was determined in all subjects and assigned to the time of isovolumetric tension. Conversely, the delay between the increase in wave amplitude and ventricular dilatation was used for measuring the time of isovolumetric elasticity relaxation.
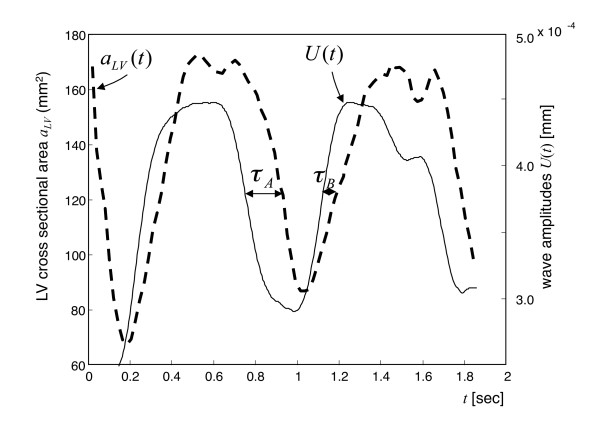
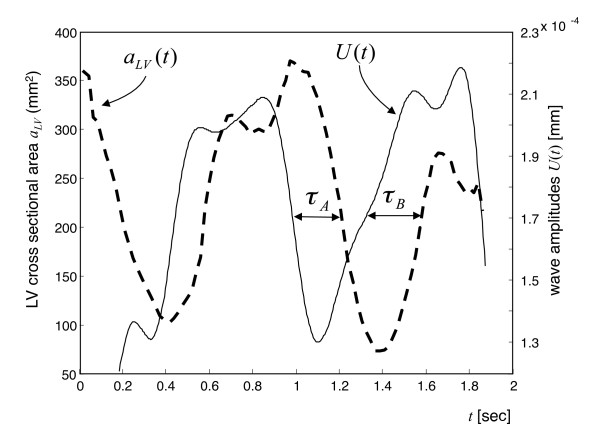
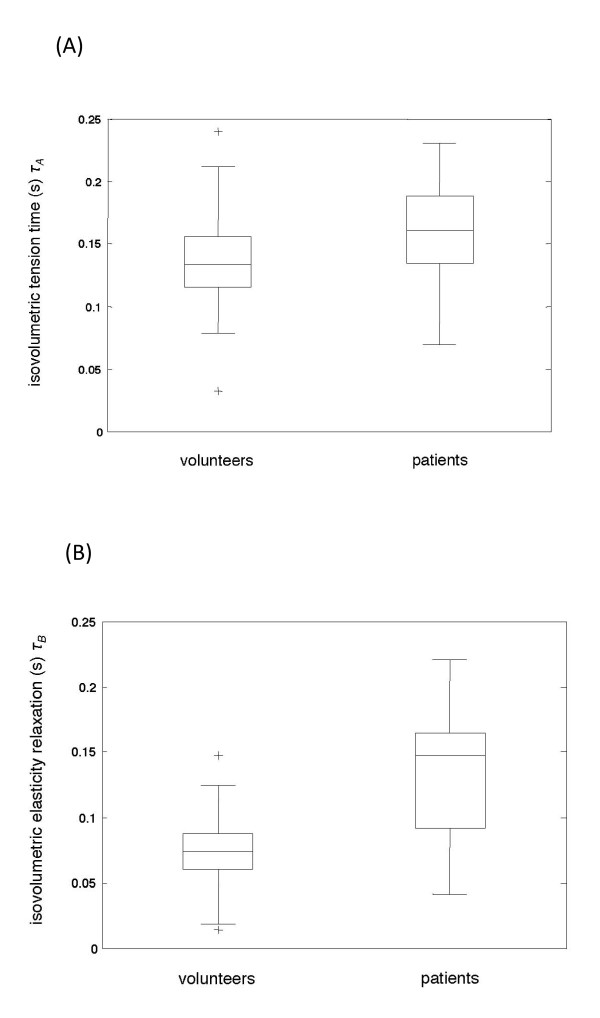
Results: Wave amplitudes decreased during systole and increased during diastole. The variation in wave amplitude occurred ahead of morphological changes. In healthy volunteers the time of isovolumetric elasticity relaxation was 75 ± 31 ms, which is significantly shorter than the time of isovolumetric tension of 136 ± 36 ms (P < 0.01). In patients with relaxation abnormalities (mild diastolic dysfunction, n = 11) isovolumetric elasticity relaxation was significantly prolonged, with 133 ± 57 ms (P < 0.01), whereas isovolumetric tension time was in the range of healthy controls (161 ± 45 ms; P = 0.053).
Conclusion: The complex MRE signal conveys complementary information on cardiac morphology and elasticity, which can be combined for directly measuring isovolumetric tension and elasticity relaxation in the human heart.
Figures
References
-
- Tei C, Ling LH, Hodge DO, Bailey KR, Oh JK, Rodeheffer RJ, Tajik AJ, Seward JB. New index of combined systolic and diastolic myocardial performance: a simple and reproducible measure of cardiac function--a study in normals and dilated cardiomyopathy. J Cardiol. 1995;26:357–366. - PubMed
-
- Cui W, Roberson DA, Chen Z, Madronero LF, Cuneo BF. Systolic and diastolic time intervals measured from Doppler tissue imaging: normal values and Z-score tables, and effects of age, heart rate, and body surface area. J Am Soc Echocardiogr. 2008;21:361–370. doi: 10.1016/j.echo.2007.05.034. - DOI - PubMed
-
- Kolipaka A, Mcgee KP, Araoz PA, Glaser KJ, Manduca A, Romano AJ, Ehman RL. MR elastography as a method for the assessment of myocardial stiffness: comparison with an established pressure-volume model in a left ventricular model of the heart. Magn Reson Med. 2009;62:135–140. doi: 10.1002/mrm.21991. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
