

Higher biologically effective dose of radiotherapy is associated with improved outcomes for locally advanced non-small cell lung carcinoma treated with chemoradiation: an analysis of the Radiation Therapy Oncology Group
- PMID: 20980108
- PMCID: PMC5764542
- DOI: 10.1016/j.ijrobp.2010.09.004
Higher biologically effective dose of radiotherapy is associated with improved outcomes for locally advanced non-small cell lung carcinoma treated with chemoradiation: an analysis of the Radiation Therapy Oncology Group
Abstract
Purpose: Patients treated with chemoradiotherapy for locally advanced non-small-cell lung carcinoma (LA-NSCLC) were analyzed for local-regional failure (LRF) and overall survival (OS) with respect to radiotherapy dose intensity.
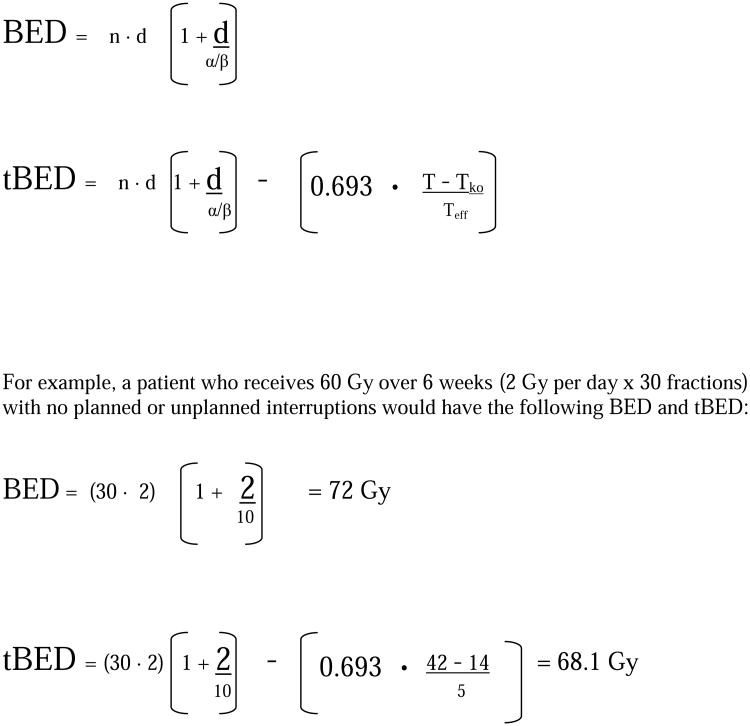
Methods and materials: This study combined data from seven Radiation Therapy Oncology Group (RTOG) trials in which chemoradiotherapy was used for LA-NSCLC: RTOG 88-08 (chemoradiation arm only), 90-15, 91-06, 92-04, 93-09 (nonoperative arm only), 94-10, and 98-01. The radiotherapeutic biologically effective dose (BED) received by each individual patient was calculated, as was the overall treatment time-adjusted BED (tBED) using standard formulae. Heterogeneity testing was done with chi-squared statistics, and weighted pooled hazard ratio estimates were used. Cox and Fine and Gray's proportional hazard models were used for OS and LRF, respectively, to test the associations between BED and tBED adjusted for other covariates.
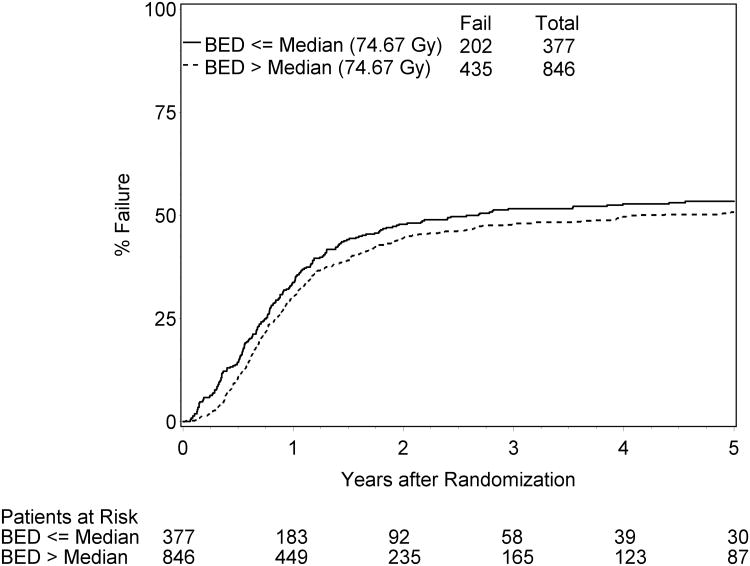
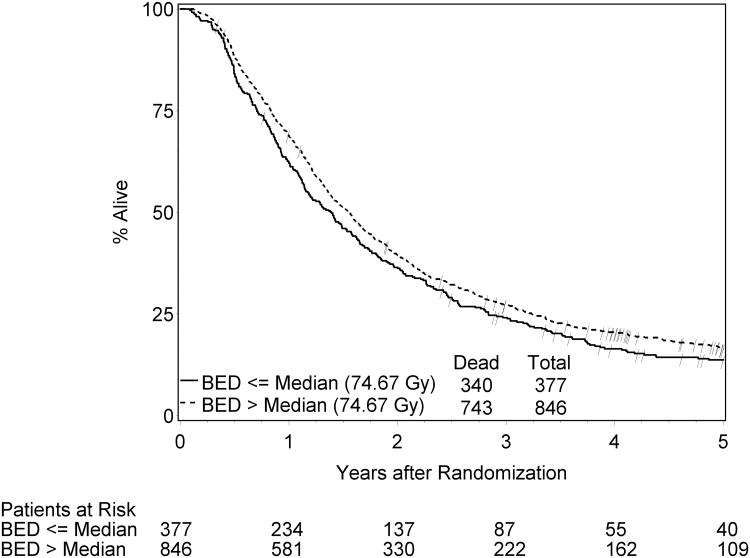
Results: A total of 1,356 patients were analyzed for BED (1,348 for tBED). The 2-year and 5-year OS rates were 38% and 15%, respectively. The 2-year and 5-year LRF rates were 46% and 52%, respectively. The BED (and tBED) were highly significantly associated with both OS and LRF, with or without adjustment for other covariates on multivariate analysis (p < 0.0001). A 1-Gy BED increase in radiotherapy dose intensity was statistically significantly associated with approximately 4% relative improvement in survival; this is another way of expressing the finding that the pool-adjusted hazard ratio for survival as a function of BED was 0.96. Similarly, a 1-Gy tBED increase in radiotherapy dose intensity was statistically significantly associated with approximately 3% relative improvement in local-regional control; this is another way of expressing the finding that the pool-adjusted hazard ratio as a function of tBED was 0.97.
Conclusions: Higher radiotherapy dose intensity is associated with improved local-regional control and survival in the setting of chemoradiotherapy.
Copyright © 2012 Elsevier Inc. All rights reserved.
Conflict of interest statement
There is no conflict of interest for any of the authors.
Figures
Comment in
-
In Regard to Machtay et al.Int J Radiat Oncol Biol Phys. 2012 Oct 1;84(2):302-3; author reply 303-4. doi: 10.1016/j.ijrobp.2012.02.046. Int J Radiat Oncol Biol Phys. 2012. PMID: 22935387 No abstract available.
References
-
- Perez CA, Pajak TF, Rubin P, et al. Long-term observations of the patterns of failure in patients with unresectable non-oat cell carcinoma of the lung treated with definitive radiotherapy. Report by the RTOG Cancer. 1987;59:1874. - PubMed
-
- Marino P, Preatoni A, Cantoni A. Randomized trials of radiotherapy alone versus combined chemotherapy and radiotherapy in stages IIIa and IIIb nonsmall cell lung cancer: A meta-analysis. Cancer. 1995;76:593–601. - PubMed
-
- Dillman RO, Herndon J, Seagren SL, Eaton WLJ, Green MR. Improved survival in stage III non-small cell lung cancer: seven-year followup of cancer and leukemia group B (CALGB) 8433 trial. J Natl Cancer Inst. 1996;88:1210–5. - PubMed
-
- Furuse K, Fukuoka M, Kawahara M. Phase III study of concurrent versus sequential thoracic radiotherapy in combination with mitomycin, vindesine, and cisplatin in unresectable stage III non-small cell lung cancer. J Clin Oncol. 1999;17:2692–9. - PubMed
-
- Machtay M, Hsu C, Komaki R, et al. Effect of overall treatment time on outcome after concurrent chemoradiation for locaclly advnced non-small cell lung carcinoma: analysis of the Radiation Therapy Oncology Group (RTOG) experience. Int J Radiat Oncol Biol Phys. 2005;63(3):667–71. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
