

In-hospital delay of elective surgery for high volume procedures: the impact on infectious complications
- PMID: 20980170
- PMCID: PMC2992590
- DOI: 10.1016/j.jamcollsurg.2010.08.009
In-hospital delay of elective surgery for high volume procedures: the impact on infectious complications
Abstract
Background: Development of infectious complications after high volume elective surgical procedures imposes a significant clinical burden to the United States population. This study evaluated the association of in-hospital delay of elective procedures and the subsequent impact on infectious complications after coronary artery bypass graft (CABG) surgery, colon resection, and lung resection.
Study design: The Nationwide Inpatient Sample was queried between 2003 and 2007, and patients who developed postoperative infectious complications were identified. Time to elective surgery in days from admission was calculated: 0, 1 day, 2 to 5 days, and 6 to 10 days. Infectious complications evaluated included pneumonia, urinary tract infections, postoperative sepsis, and surgical site infections. Chi-square, multivariable logistic regression analyses, analysis of variance, and Cochran-Armitage trend test were used.
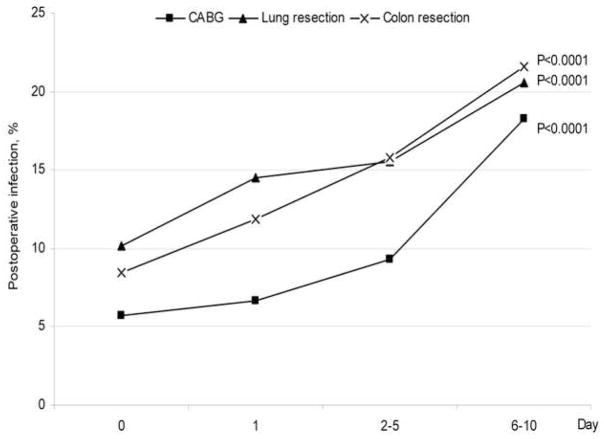
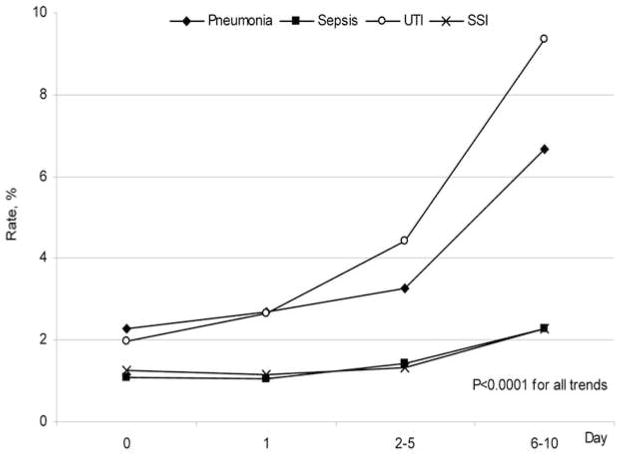
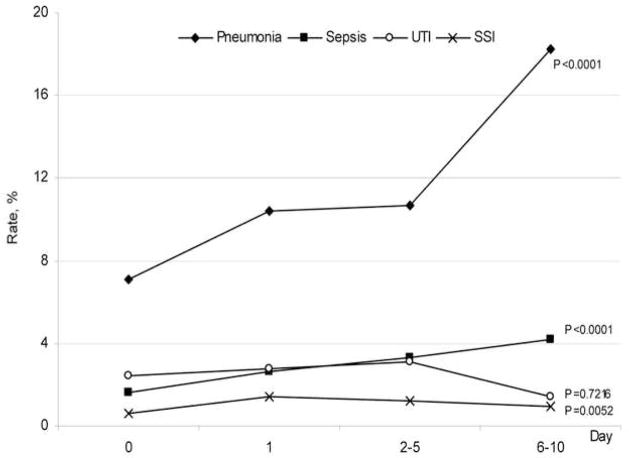
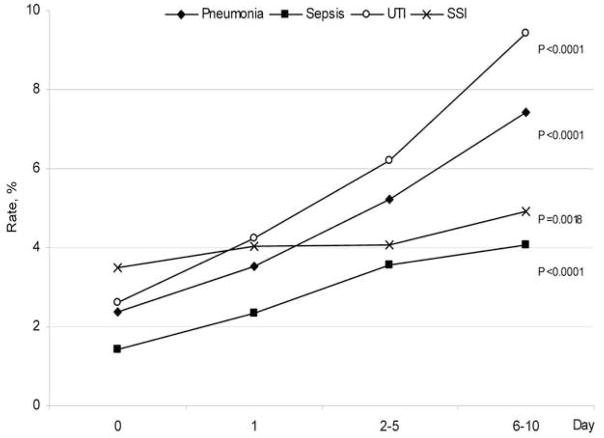
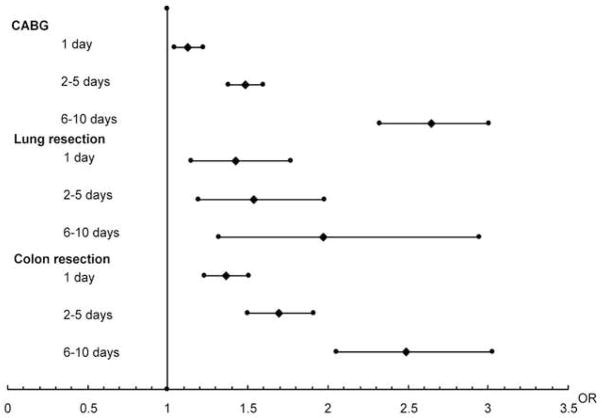
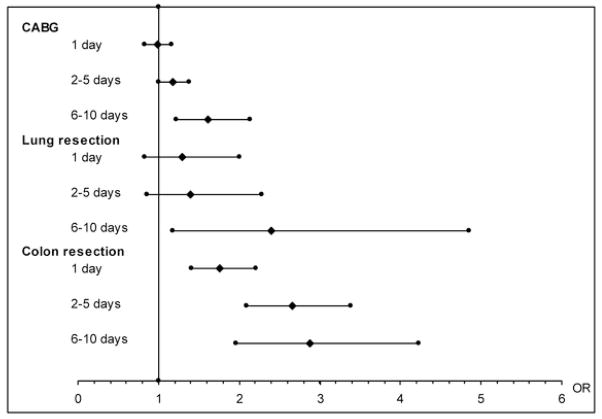
Results: There were 87,318 CABG procedures, 46,728 colon resections, and 28,960 lung resections evaluated. Total infection rates significantly increased after elective surgery delays: CABG: 0 days, 5.73%;1 day, 6.68%; 2 to 5 days, 9.33%; 6 to 10 days,18.24%; colon resections: 0 days, 8.43 %;1 day, 11.86%; 2 to 5 days,15.79%;6 to 10 days,21.62%; and lung resections: 0 days, 10.17%;1 day, 14.53%; 2 to 5 days, 15.53%; 6 to 10 days, 20.56%, p < 0.0001 for all trends. Trends for increasing infections after delay were significant for pneumonia and sepsis for all procedures (p < 0.0001); urinary tract infections and surgical site infections significantly increased after CABG and colon resection. Age 80 years and older, female gender, black and Hispanic race or ethnicity, and comorbidities including congestive heart failure, chronic pulmonary disease, and renal failure were associated with delay in surgery. Postoperative hospital mortality after delayed procedures was also greater. Mean cost increased after all procedures with delays: CABG, from $25,164 to $42,055 (p < 0.0001); colon resections, from $13,660 to $25,307) (p < 0.0001); and lung resections, from $18,519 to $25,054 (p < 0.0001).
Conclusions: In-hospital delay of elective surgery from the day of admission was associated with a significant increase in infectious complications and mortality. This delay was also associated with a significant increase in hospital cost. Future policy directed toward preventing in-hospital delay of elective surgery may offer significant cost savings and decrease infectious complications after elective surgery.
Copyright © 2010 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Saez-Castillo AJ, Olmo-Jimenez MJ, Perez Sanchez JM, et al. Bayesian Analysis of Nosocomial Infection Risk and Length of Stay in a Department of General and Digestive Surgery. Value Health. 2010 - PubMed
-
- Vogel TR, Dombrovskiy VY, Carson JL, et al. Infectious complications after elective vascular surgical procedures. J Vasc Surg. 2010;51:122–9. discussion 129–130. - PubMed
-
- Fry DE. A systems approach to the prevention of surgical infections. Surg Clin North Am. 2009;89:521–537. x. - PubMed
-
- Dimick JB, Chen SL, Taheri PA, et al. Hospital costs associated with surgical complications: a report from the private-sector National Surgical Quality Improvement Program. J Am Coll Surg. 2004;199:531–537. - PubMed
-
- Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36:8–27. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
