

Total laparoscopic conservative surgery for an intramural ectopic pregnancy
- PMID: 20981282
- PMCID: PMC2963121
- DOI: 10.1155/2010/504062
Total laparoscopic conservative surgery for an intramural ectopic pregnancy
Abstract
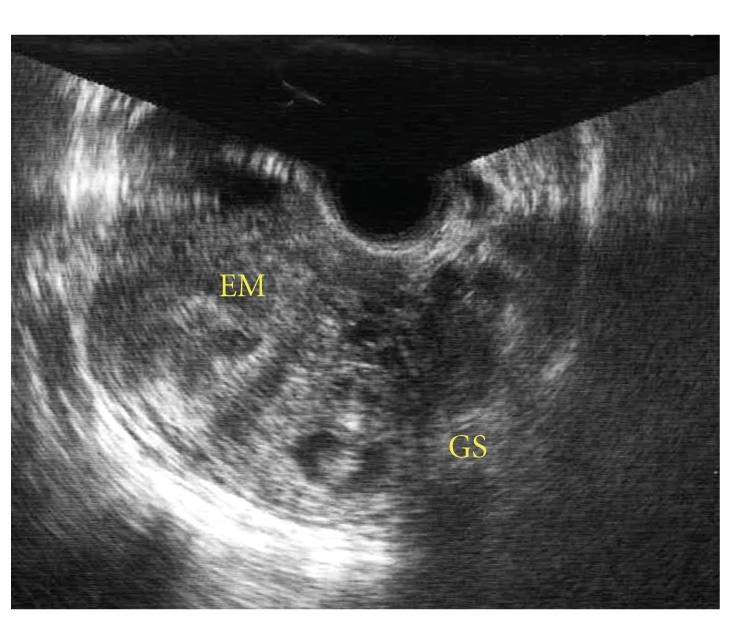
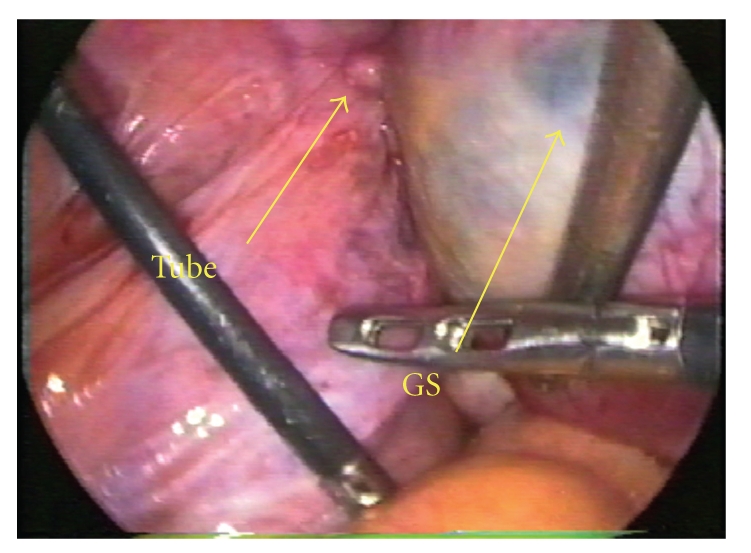
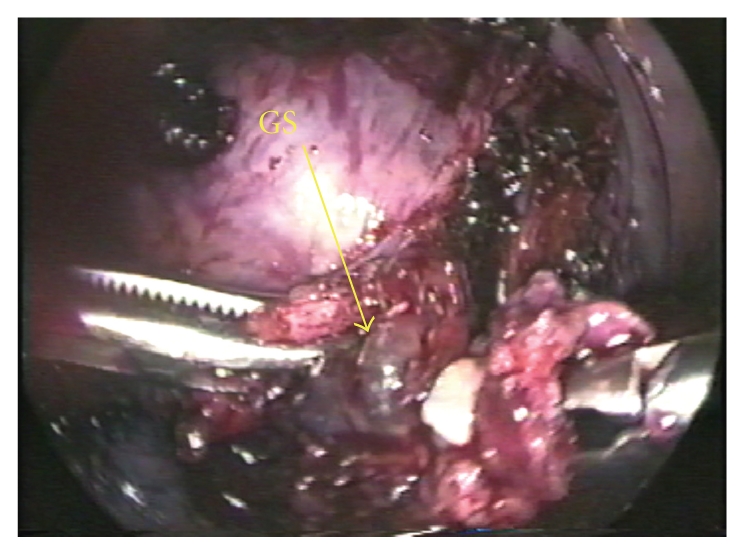
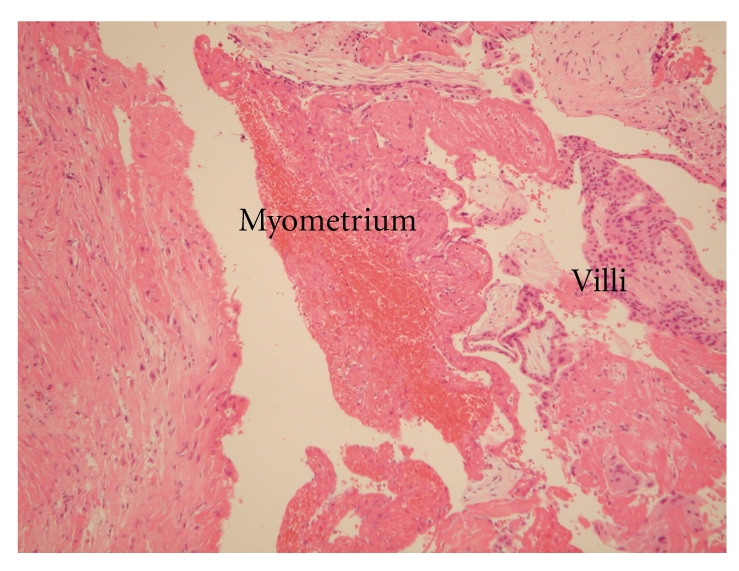
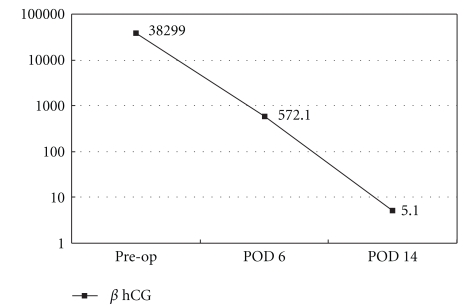
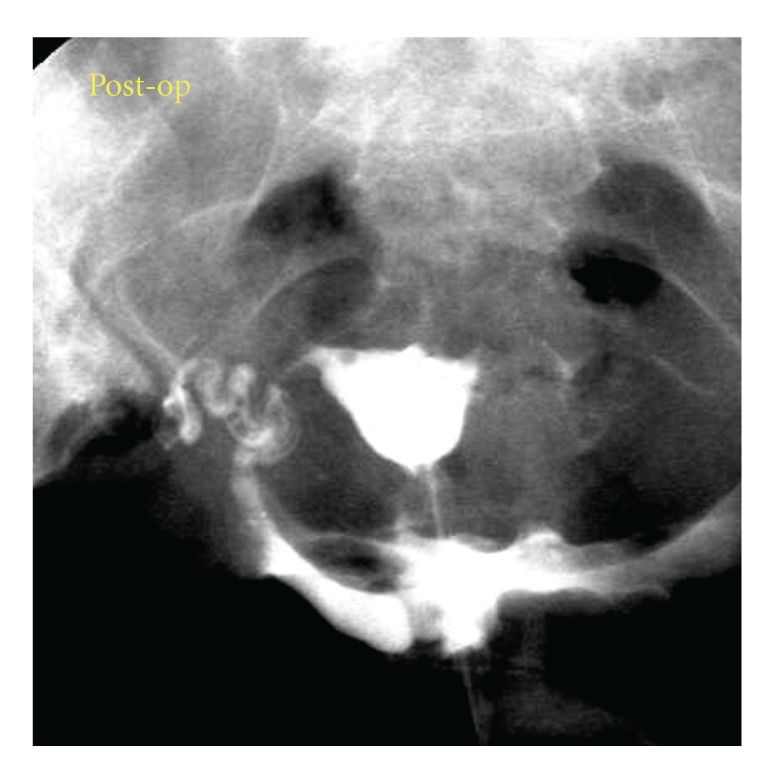
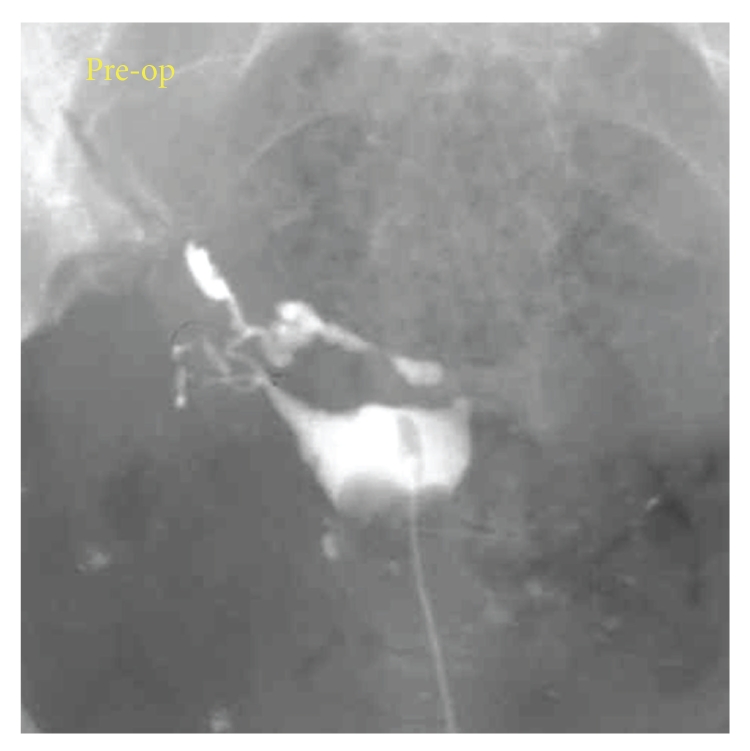
A 38-year-old woman, gravida 3, para 1 with a history of a left salpingectomy for an ectopic pregnancy was admitted for treatment of a presumed ectopic pregnancy. Transvaginal sonography revealed an ill-defined gestational sac and fetal heart beat within the fundal myometrium adjacent to the left cornua. Laparoscopy was performed for a suspected left cornual pregnancy or intramural pregnancy. A cystic mass 3 cm in diameter was visible within the fundal myometrium. Total laparoscopic removal of the gestational sac was performed, and the uterus was preserved. Pathologic evaluation of the excised mass demonstrated chorionic villi involving the myometrium. In the literature, only one other case describing the laparoscopic removal of an intramural pregnancy has been reported. However, in the prior report, the patient still required hysterectomy after conservative surgery. Therefore, this is the first report of the successful treatment of an intramural pregnancy exclusively with laparoscopy.
Figures
Similar articles
-
Intramural pregnancy: a report of 2 cases.J Reprod Med. 2004 Jul;49(7):569-72. J Reprod Med. 2004. PMID: 15305831
-
Decidualized juvenile cystic adenomyoma mimicking a cornual pregnancy.Fertil Steril. 2020 Feb;113(2):463-465. doi: 10.1016/j.fertnstert.2019.10.026. Fertil Steril. 2020. PMID: 32106998
-
Hysteroscopy-assisted laparoscopic salpingectomy for interstitial pregnancy without cornual resection.Fertil Steril. 2021 Sep;116(3):909-911. doi: 10.1016/j.fertnstert.2021.05.082. Epub 2021 Jun 9. Fertil Steril. 2021. PMID: 34116833
-
Minimally invasive management of intramural pregnancy using ultrasound combined with laparoscopy -based learning experience from a low-middle income country: a case report and review of the literature.J Med Case Rep. 2024 Dec 3;18(1):593. doi: 10.1186/s13256-024-04966-6. J Med Case Rep. 2024. PMID: 39627878 Free PMC article. Review.
-
Intramural ectopic pregnancy following pelvic adhesion: case report and literature review.Arch Gynecol Obstet. 2019 Dec;300(6):1507-1520. doi: 10.1007/s00404-019-05379-3. Epub 2019 Nov 15. Arch Gynecol Obstet. 2019. PMID: 31729562 Review.
Cited by
-
Intramural ectopic pregnancy: An individual patient data systematic review.Eur J Obstet Gynecol Reprod Biol X. 2023 Dec 20;21:100272. doi: 10.1016/j.eurox.2023.100272. eCollection 2024 Mar. Eur J Obstet Gynecol Reprod Biol X. 2023. PMID: 38269031 Free PMC article. Review.
-
Incidence, diagnosis and management of tubal and nontubal ectopic pregnancies: a review.Fertil Res Pract. 2015 Oct 15;1:15. doi: 10.1186/s40738-015-0008-z. eCollection 2015. Fertil Res Pract. 2015. PMID: 28620520 Free PMC article. Review.
-
Intramyometrial pregnancy after cryopreserved embryo transfer: a case report.BMC Pregnancy Childbirth. 2020 Feb 10;20(1):90. doi: 10.1186/s12884-020-2784-7. BMC Pregnancy Childbirth. 2020. PMID: 32041575 Free PMC article.
-
[Intramural ectopic pregnancy: about a case].Pan Afr Med J. 2015 Jul 24;21:217. doi: 10.11604/pamj.2015.21.217.7274. eCollection 2015. Pan Afr Med J. 2015. PMID: 26448812 Free PMC article. French.
-
Management of interstitial pregnancy in the era of laparoscopy: a meta-analysis of 855 case studies compared with traditional techniques.Obstet Gynecol Sci. 2021 Mar;64(2):156-173. doi: 10.5468/ogs.20299. Epub 2021 Feb 4. Obstet Gynecol Sci. 2021. PMID: 33539687 Free PMC article.
References
-
- McGowan L. Intramural pregnancy. The Journal of the American Medical Association. 1965;192(7):637–638. - PubMed
-
- Tucker SW. Laparoscopic management of an intramural pregnancy. Journal of the American Association of Gynecologic Laparoscopists. 1995;2(4):467–470. - PubMed
-
- Gleicher N, Karande V, Rabin D, Pratt D. Laparoscopic removal of twin cornual pregnancy after in vitro fertilization. Fertility and Sterility. 1994;61(6):1161–1162. - PubMed
-
- Kojima E, Abe Y, Morita M, Ito M, Hirakawa S, Momose K. The treatment of unruptured tubal pregnancy with intratubal methotrexate injection under laparoscopic control. Obstetrics and Gynecology. 1990;75(4):723–725. - PubMed
-
- Okonofua FE, Ojo OS, Odunsi OA, Odesanmi WO. Ectopic pregnancy associated with tubal schistosomiasis in a Nigerian woman. International Journal of Gynecology and Obstetrics. 1990;32(3):281–284. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
