

Scleroderma renal crisis: a pathology perspective
- PMID: 20981312
- PMCID: PMC2958499
- DOI: 10.1155/2010/543704
Scleroderma renal crisis: a pathology perspective
Abstract
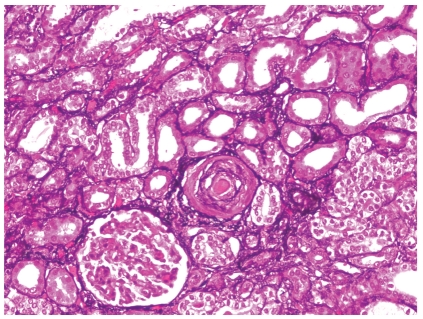
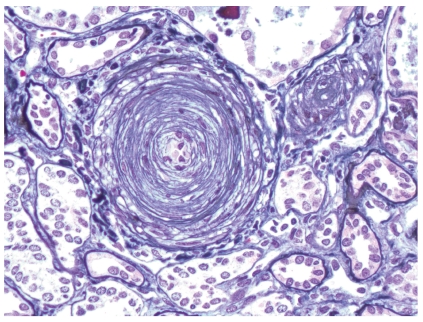
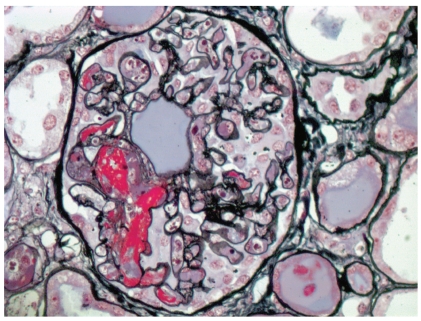
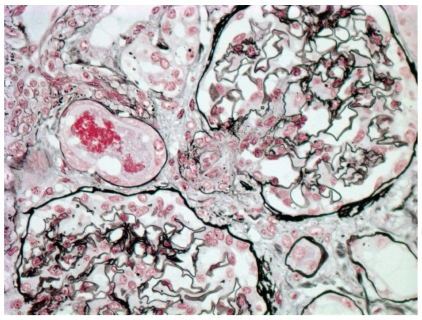
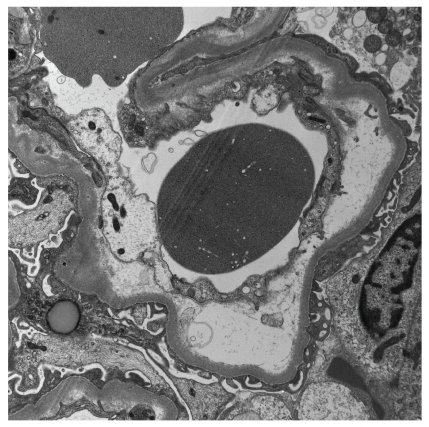
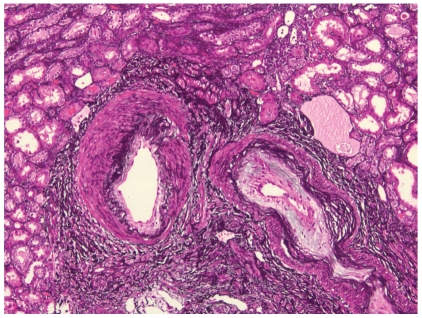
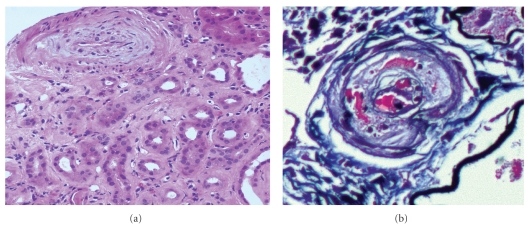
Scleroderma renal crisis (SRC) is an infrequent but serious complication of systemic sclerosis (SSc). It is associated with increased vascular permeability, activation of coagulation cascade, and renin secretion, which may lead to the acute renal failure typically associated with accelerated hypertension. The histologic picture of SRC is that of a thrombotic microangiopathy process with prominent small vessel involvement manifesting as myxoid intimal changes, thrombi, onion skin lesions, and/or fibrointimal sclerosis. Renal biopsies play an important role in confirming the clinical diagnosis, excluding overlapping/superimposed diseases that might lead to acute renal failure in SSc patients, helping to predict the clinical outcome and optimizing patient management. Kidney transplantation may be the only treatment option available for a subset of SRC patients who develop end-stage renal failure despite aggressive angiotensin-converting enzyme inhibitor therapy. However, the posttransplant outcome for SSc patients is currently suboptimal compared to the general renal transplant population.
Figures
Similar articles
-
Scleroderma renal crisis and renal involvement in systemic sclerosis.Nat Rev Nephrol. 2016 Nov;12(11):678-691. doi: 10.1038/nrneph.2016.124. Epub 2016 Sep 19. Nat Rev Nephrol. 2016. PMID: 27641135 Review.
-
Scleroderma renal crisis in a case of mixed connective tissue disease.Saudi J Kidney Dis Transpl. 2014 Jul;25(4):844-8. doi: 10.4103/1319-2442.135177. Saudi J Kidney Dis Transpl. 2014. PMID: 24969199 Review.
-
De novo normotensive scleroderma renal crisis six years after living-donor renal transplantation in a patient with overlapping systemic sclerosis/systemic lupus erythematosus syndrome: a case report.BMC Nephrol. 2023 Dec 4;24(1):355. doi: 10.1186/s12882-023-03416-7. BMC Nephrol. 2023. PMID: 38049714 Free PMC article.
-
Scleroderma renal crisis during intravenous cyclophosphamide pulse therapy for complicated interstitial lung disease was successfully treated with angiotensin converting enzyme inhibitor and plasma exchange.Nagoya J Med Sci. 2016 Aug;78(3):329-34. Nagoya J Med Sci. 2016. PMID: 27578917 Free PMC article.
-
Systemic sclerosis complicated with renal thrombotic microangiopathy: a case report and literature review.BMC Nephrol. 2022 Jan 10;23(1):22. doi: 10.1186/s12882-021-02639-w. BMC Nephrol. 2022. PMID: 35012481 Free PMC article. Review.
Cited by
-
A Narrative Review of Pathogenetic and Histopathologic Aspects, Epidemiology, Classification Systems, and Disease Outcome Measures in Systemic Sclerosis.Clin Rev Allergy Immunol. 2023 Jun;64(3):358-377. doi: 10.1007/s12016-022-08929-x. Epub 2022 Mar 7. Clin Rev Allergy Immunol. 2023. PMID: 35254622 Free PMC article. Review.
-
Scleroderma Renal Crisis Associated With Microangiopathic Hemolytic Anemia in a Patient With Seronegative Scleroderma and Monoclonal Gammopathy.J Investig Med High Impact Case Rep. 2022 Jan-Dec;10:23247096221074591. doi: 10.1177/23247096221074591. J Investig Med High Impact Case Rep. 2022. PMID: 35152792 Free PMC article.
-
Evaluation of hypertension in systemic sclerosis and systemic lupus erythematosus overlap.J Scleroderma Relat Disord. 2023 Feb;8(1):14-19. doi: 10.1177/23971983221122673. Epub 2022 Sep 14. J Scleroderma Relat Disord. 2023. PMID: 36743818 Free PMC article. Review.
-
Kidney involvement in systemic sclerosis: From pathogenesis to treatment.J Scleroderma Relat Disord. 2018 Feb;3(1):43-52. doi: 10.1177/2397198318758607. Epub 2018 Apr 4. J Scleroderma Relat Disord. 2018. PMID: 35382123 Free PMC article. Review.
-
Scleroderma Renal Crisis in a Normotensive Patient.Kidney Int Rep. 2016 Jul 25;1(4):311-315. doi: 10.1016/j.ekir.2016.07.005. eCollection 2016 Nov. Kidney Int Rep. 2016. PMID: 29318207 Free PMC article. No abstract available.
References
-
- Sakkas LI. New developments in the pathogenesis of systemic sclerosis. Autoimmunity. 2005;38(2):113–116. - PubMed
-
- Sugimoto T, Sanada M, Kashiwagi A. Is scleroderma renal crisis with anti-centromere antibody-positive limited cutaneous systemic sclerosis overlooked in patients with hypertension and/or renal dysfunction? Nephrology. 2008;13(2):179–180. - PubMed
-
- Sugimoto T, Soumura M, Danno K, et al. Scleroderma renal crisis in a patient with anticentromere antibody-positive limited cutaneous systemic sclerosis. Modern Rheumatology. 2006;16(5):309–311. - PubMed
-
- Gonzalez EA, Schmulbach E, Bastani B. Scleroderma renal crisis with minimal skin involvement and no serologic evidence of systemic sclerosis. American Journal of Kidney Diseases. 1994;23(2):317–319. - PubMed
-
- Chizzolini C. Update on pathophysiology of scleroderma with special reference to immunoinflammatory events. Annals of Medicine. 2007;39(1):42–53. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
