

Evaluation of a magnetic resonance-compatible dentoalveolar tactile stimulus device
- PMID: 21029454
- PMCID: PMC2988799
- DOI: 10.1186/1471-2202-11-142
Evaluation of a magnetic resonance-compatible dentoalveolar tactile stimulus device
Abstract
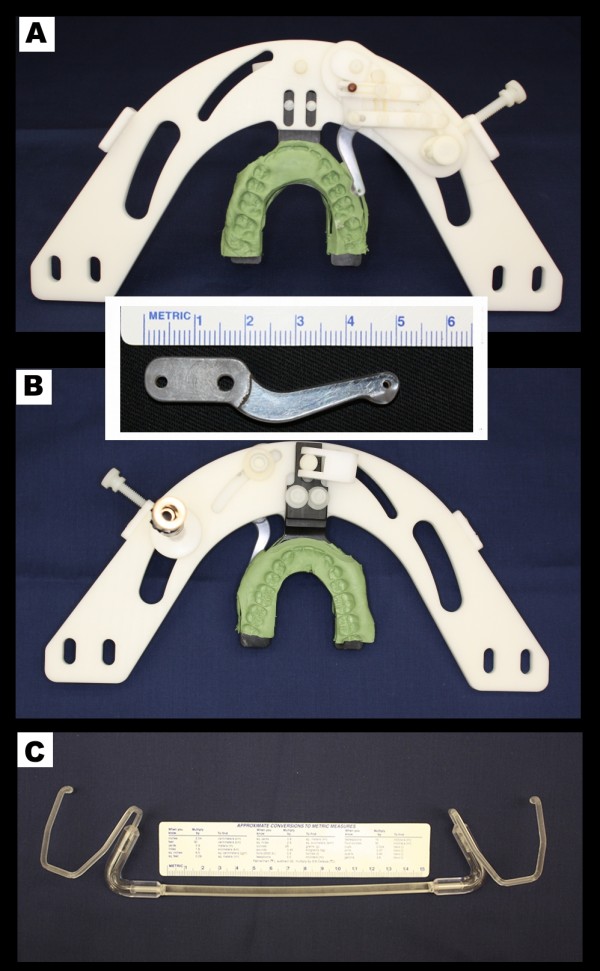
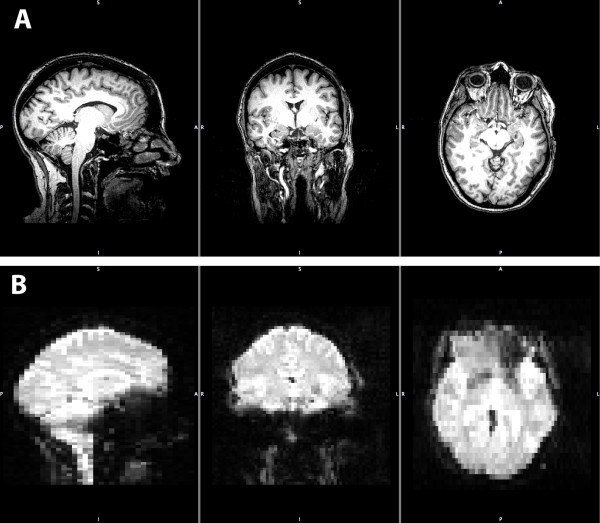
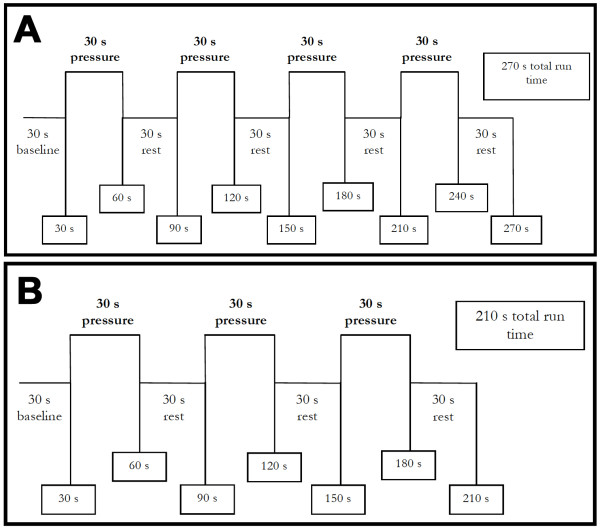
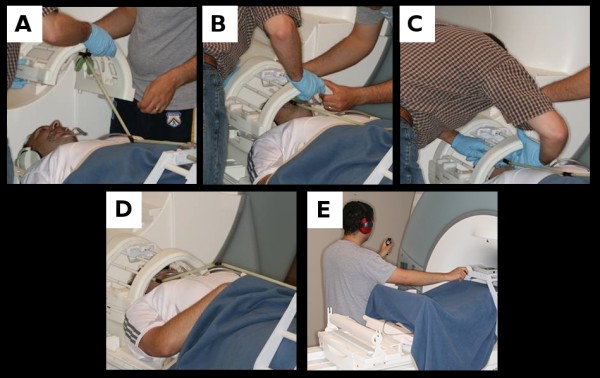
Background: Few methods exist to study central nervous system processes following dentoalveolar tactile stimulation using functional magnetic resonance imaging (fMRI), likely due to inherent technical difficulties. Our primary goal was to develop and perform feasibility testing of a novel device capable of delivering valid and reliable dentoalveolar stimuli at dental chair-side and during MRI. Details of a device designed to deliver dentoalveolar dynamic pressure stimuli are described. Device testing took place in three settings: a) laboratory testing to assess range of stimulus force intensities, b) dental chair-side to assess reliability, validity and discriminant ability in force-pain relationship; and c) MRI to evaluate magnetic compatibility and ability to evoke brain activation in painfree subjects similar to those described in the literature.
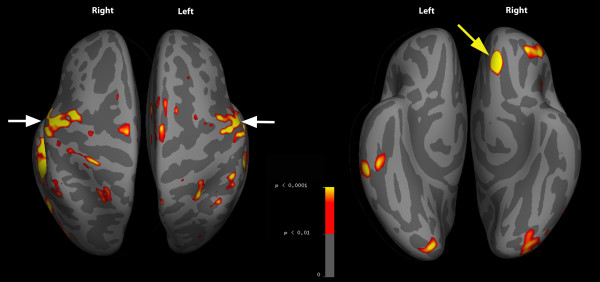
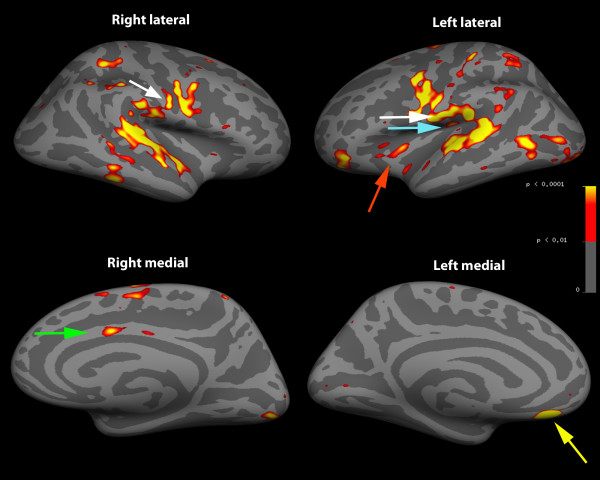
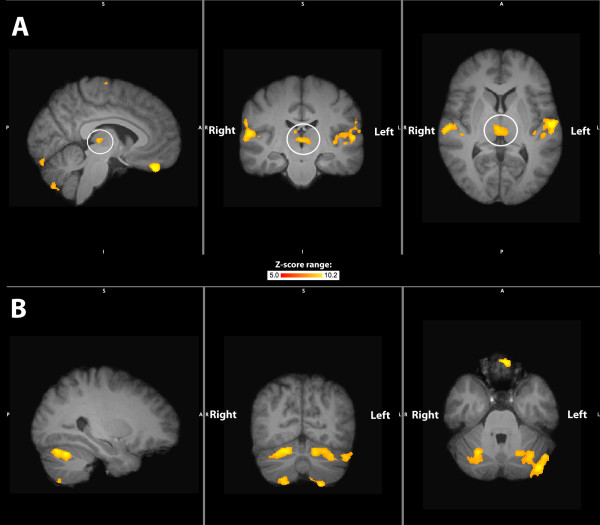
Results: A novel device capable of delivering valid and reliable dentoalveolar somatosensory stimulation was developed (ICC = 0.89, 0.78-1 [95% CI]). Psychophysical data analysis showed high discriminant ability in differentiating painfree controls from cases with chronic dentoalveolar pain related to deafferenting dental procedures (sensitivity = 100%, specificity = 86.7%, area under ROC curve = 0.99). FMRI results of dentoalveolar dynamic pressure pain in painfree subjects revealed activation of brain areas typically associated with acute pain processing including thalamus, primary/secondary somatosensory, insular and prefrontal cortex.
Conclusions: A novel psychophysical method to deliver dynamic dentoalveolar pressure stimulation was developed and validated, allowing non-invasive MRI-based exploration of central nervous system function in response to intraoral somatosensation.
Background: The organization of the trigeminal system is unique as it provides somatosensory innervation to the face, masticatory and oral structures, the majority of the intracranial contents 1 and to specialized structures (tongue, nasal mucosa, auricle, tympanic membrane, cornea and part of the conjunctiva) 2. Somatic sensory information transmitted by the trigeminal nerve is crucial for normal orofacial function; however, the mechanisms of many chronic pain conditions affecting areas innervated by this sensory system are not well understood 345. The clinical presentation of chronic intraoral pain in the area of a tooth or in a site formally occupied by a tooth with no clinical or radiological signs of pathology, referred to as atypical odontalgia (AO) 67, is one such chronic pain condition of particular interest to dentists that is difficult to diagnose and manage. Recent research suggests both peripheral and central nervous system mechanisms being involved in AO pathophysiology 8910, but the majority of mechanism-based research of patients with AO has focused on the "peripheral aspect" 7.Functional magnetic resonance imaging (fMRI) is an established research technique to study the central aspects of pain 11. Of existing neuroimaging techniques, fMRI provides good spatial resolution of cortical and subcortical structures critical in the processing of nociception, acceptable temporal resolution, does not involve ionizing radiation, and can be performed using most MRI systems that already exist in research centers and the community. For these reasons, we sought to develop a protocol that allows us to use this tool to investigate the central mechanisms involved in the processes of intraoral pain arising from the dentoalveolar region. Using this device, our long-term objective is to improve our understanding of the underlying mechanisms of persistent dentoalveolar pain.In the past few years several studies used fMRI to investigate the human trigeminal system 1213, with a limited subset focusing on intraoral stimulation - specifically on the dentoalveolar processes, such as lip, tongue and teeth stimulation 14 or only teeth 151617. Some reasons for scarce literature on this topic may be the technical challenges involved in delivering facial/intraoral stimulation inside a MR scanner 1718: possibility of magnetic interference, detriment of image quality, subject discomfort and reduced working space between the subject's head and the radiofrequency coil. As a consequence a MR-compatible device would need to not only overcome these challenges but also be capable of delivering a controlled and reproducible stimuli 19, as reliability/reproducibility is a necessary feature of sensory testing 20.Existing MR-compatible methods of dentoalveolar stimulation are limited and do not adequately deliver stimuli across a range of non-painful to painful intensities and/or cannot be adjusted to reach posterior aspects of the dentoalveolar region. Therefore our goal was to develop and test the feasibility of a device able to: 1) provide reliable and valid dentoalveolar stimuli, 2) deliver such stimulation within the restricted space of an MR head coil, 3) be compatible for use within an MR environment, and 4) produce brain activation in painfree controls consistent to those observed by others using fMRI.
Figures
References
-
- Moore KL, Dalley AF, Agur AMR. Clinically oriented anatomy. 5. Baltimore, MD: Lippincott Williams & Wilkins; 2006.
-
- Woda A, Pionchon P. A unified concept of idiopathic orofacial pain: clinical features. J Orofac Pain. 1999;13(3):172–184. discussion 185-195. - PubMed
-
- Woda A, Pionchon P. A unified concept of idiopathic orofacial pain: pathophysiologic features. J Orofac Pain. 2000;14(3):196–212. - PubMed
-
- Lavigne G, Woda A, Truelove E, Ship JA, Dao T, Goulet JP. Mechanisms associated with unusual orofacial pain. J Orofac Pain. 2005;19(1):9–21. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
