

The impact of emergency medical services on the ED care of severe sepsis
- PMID: 21030181
- PMCID: PMC3032016
- DOI: 10.1016/j.ajem.2010.09.015
The impact of emergency medical services on the ED care of severe sepsis
Abstract
Objective: The identification and treatment of critical illness is often initiated by emergency medical services (EMS) providers. We hypothesized that emergency department (ED) patients with severe sepsis who received EMS care had more rapid recognition and treatment compared to non-EMS patients.
Methods: This was a prospective observational study of ED patients with severe sepsis treated with early goal-directed therapy (EGDT).We included adults with suspected infection, evidence of systemic inflammation, and either hypotension after a fluid bolus or elevated lactate. Prehospital and ED clinical variables and outcomes data were collected. The primary outcome was time to initiation of antibiotics in the ED.
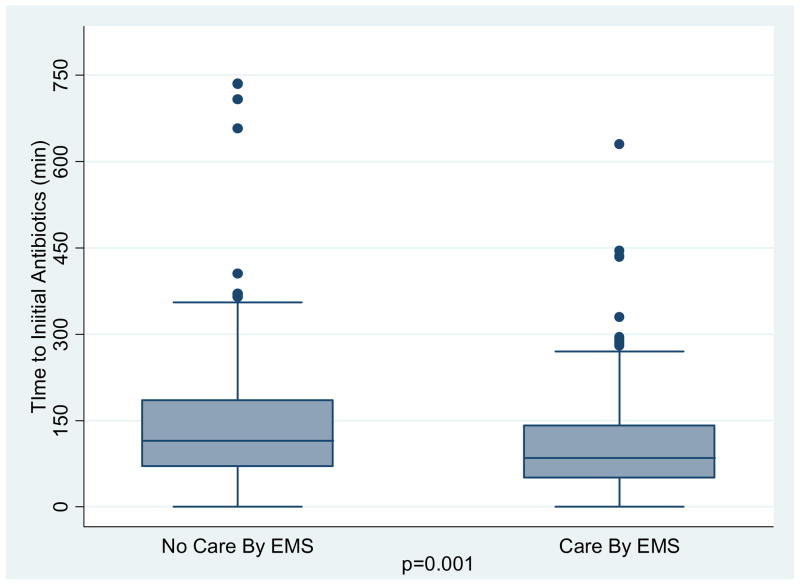
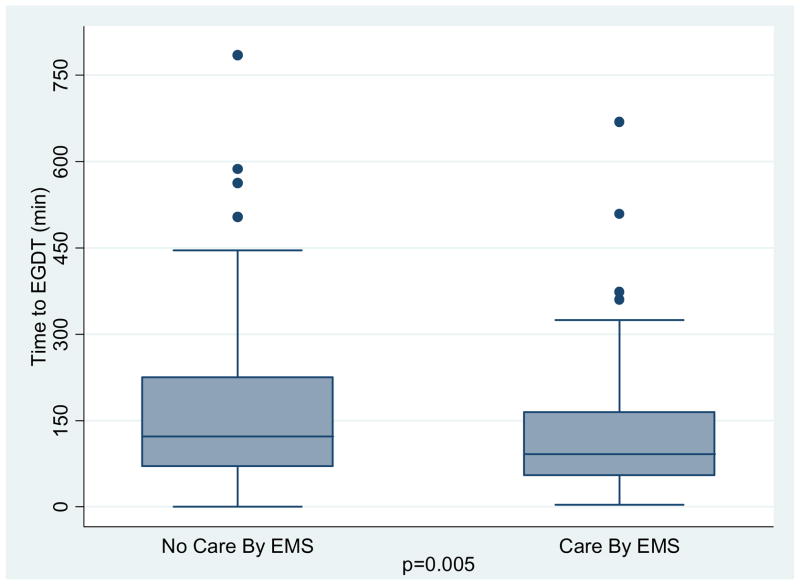
Results: There were 311 patients, with 160 (51.4%) transported by EMS. Emergency medical services-transported patients had more organ failure (Sequential Organ Failure Assessment score, 7.0 vs 6.1; P = .02), shorter time to first antibiotics (111 vs 146 minutes, P = .001), and shorter time from triage to EGDT initiation (119 vs 160 minutes, P = .005) compared to non-EMS-transported patients. Among EMS patients, if the EMS provider indicated a written impression of sepsis, there was a shorter time to antibiotics (70 vs 122 minutes, P = .003) and a shorter time to EGDT initiation (69 vs 131 minutes, P = .001) compared to those without an impression of sepsis.
Conclusions: In this prospective cohort, EMS provided initial care for half of the patients with severe sepsis requiring EGDT. Patients presented by EMS had more organ failure and a shorter time to both antibiotic and EGDT initiation in the ED.
Copyright © 2012 Elsevier Inc. All rights reserved.
Figures
References
-
- Angus D, Linde-Zwirble W, Lidicker J, et al. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001 July;29(7):1303–10. - PubMed
-
- Wang HE, Shapiro NI, Angus DC, et al. National estimates of severe sepsis in United States emergency departments. Crit Care Med. 2007;35:1928–36. - PubMed
-
- Dellinger RP, Levy MM, Carlet JM, et al. Surviving sepsis campaign: International guidelines for management of severe sepsis and septic shock: 2008. Crit Care Med. 2008;36:296–327. - PubMed
-
- Kumar A, Roberts D, Wood KE, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006 June;34:1589–96. - PubMed
