

Thirty-day mortality and late survival with reinterventions and readmissions after open and endovascular aortic aneurysm repair in Medicare beneficiaries
- PMID: 21030195
- PMCID: PMC3010445
- DOI: 10.1016/j.jvs.2010.08.051
Thirty-day mortality and late survival with reinterventions and readmissions after open and endovascular aortic aneurysm repair in Medicare beneficiaries
Abstract
Objectives: Late survival is similar after open and endovascular abdominal aortic aneurysm (AAA) repair (EVAR), despite a perioperative benefit with EVAR. AAA-related reinterventions are more common after EVAR, whereas laparotomy-related reinterventions are more common after open repair. The effect of reinterventions on survival, however, is unknown. We therefore evaluated the rate of reinterventions and readmission after initial AAA repair, 30-day mortality, and the effect on long-term survival.
Methods: We identified AAA-related and laparotomy-related reinterventions for propensity score-matched cohorts of 45,652 Medicare beneficiaries undergoing EVAR and open repair from 2001 to 2004. Follow-up was up to 6 years. Hospitalizations for ruptured AAA without repair and for bowel obstruction or ventral hernia without abdominal surgery were also recorded. Event rates were calculated per year and are presented through 6 years of follow-up as events per 100 person-years. Thirty-day mortality was calculated for each reintervention or readmission.
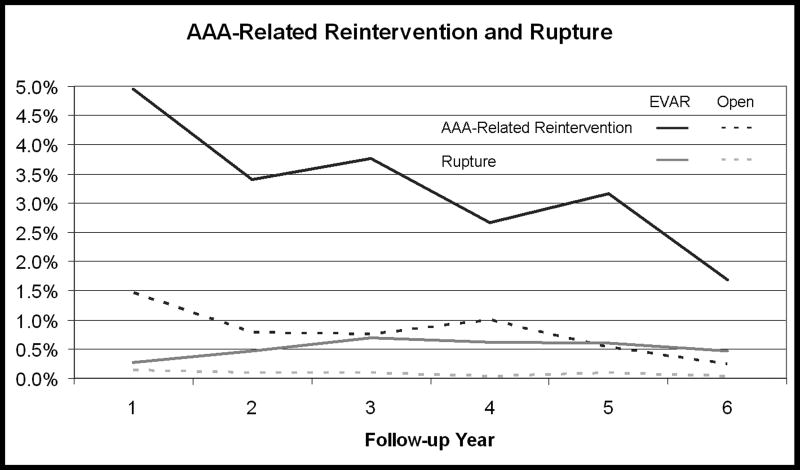
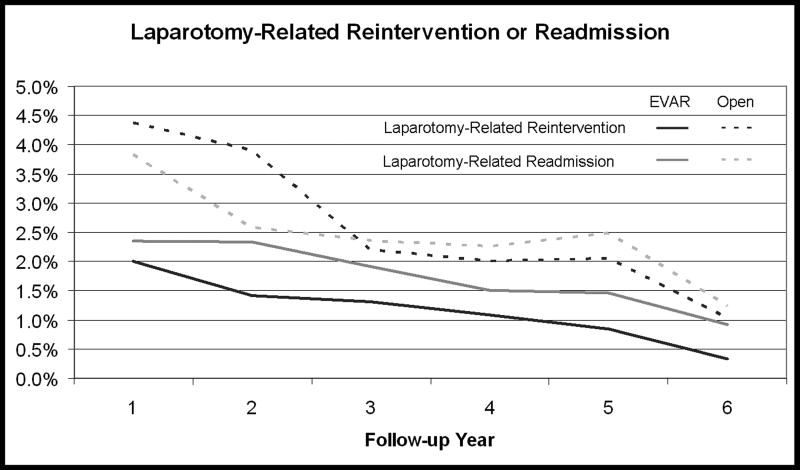
Results: Through 6 years, overall reinterventions or readmissions were similar between repair methods but slightly more common after EVAR (7.6 vs 7.0/100 person-years; relative risk [RR], 1.1; P < .001). Overall 30-day mortality with any reintervention or readmission was 9.1%. EVAR patients had more ruptures (0.50 vs 0.09 [RR, 5.7; P < .001]), with a mortality of 28%, but these were uncommon. EVAR patients also had more AAA-related reinterventions through 6 years (3.7 vs 0.9 [RR, 4.0; P < .001]; mortality, 5.6%), most of which were minor endovascular reinterventions (2.4 vs 0.2 [RR, 11.4; P < .001]), with a 30-day mortality of 3.0%. However, minor open (0.8 vs 0.5 [RR, 1.4; P < .001]; mortality, 6.9%) and major reinterventions (0.4 vs 0.2 [RR, 2.4; P < .001]; mortality, 12.1%) were also more common after EVAR than open repair. Conversely, EVAR patients had fewer laparotomy-related reinterventions than open patients (1.4 vs 3.0 [RR, 0.5; P < .001]; mortality, 8.1%) and readmissions without surgery (2.0 vs 2.7 [RR, 0.7; P < .001]; mortality 10.9%). Overall, reinterventions or readmission accounted for 9.6% of all EVAR deaths and 7.6% of all open repair deaths in the follow-up period (P < .001).
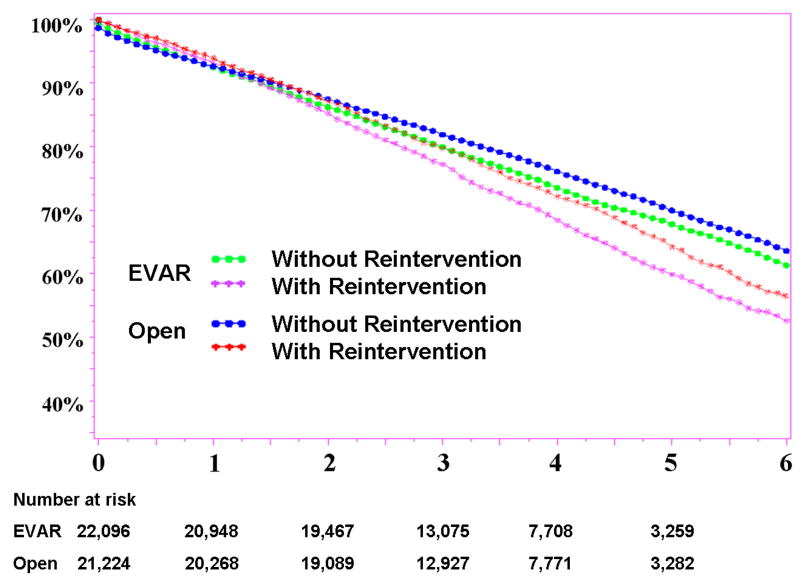
Conclusions: Reintervention and readmission are slightly higher after EVAR. Survival is negatively affected by reintervention or readmission after EVAR and open surgery, which likely contributes to the erosion of the survival benefit of EVAR over time.
Copyright © 2011 Society for Vascular Surgery. Published by Mosby, Inc. All rights reserved.
Figures
Comment in
-
Invited commentary.J Vasc Surg. 2011 Jan;53(1):13. doi: 10.1016/j.jvs.2010.08.052. J Vasc Surg. 2011. PMID: 21184930 No abstract available.
References
-
- Schermerhorn ML, O'Malley AJ, Jhaveri A, Cotterill P, Pomposelli F, Landon BE. Endovascular vs. Open Repair of Abdominal Aortic Aneurysms in the Medicare Population. N Engl J Med. 2008;358:464–74. - PubMed
-
- EVAR Trial Participants. Endovascular aneurysm repair versus open repair in patients with abdominal aortic aneurysm (EVAR trial 1): randomised controlled trial. The Lancet. 365:2179–86. - PubMed
-
- Blankensteijn JD, de Jong SECA, Prinssen M, van der Ham AC, Buth J, van Sterkenburg SM, et al. Two-Year Outcomes after Conventional or Endovascular Repair of Abdominal Aortic Aneurysms. N Engl J Med. 2005;352:2398–405. - PubMed
-
- Greenhalgh RM, Brown LC, Kwong GP, Powell JT, Thompson SG, EVAR trial participants Comparison of endovascular aneurysm repair with open repair in patients with abdominal aortic aneurysm (EVAR trial 1), 30-day operative mortality results: randomised controlled trial. Lancet. 364:843–8. - PubMed
-
- Prinssen M, Verhoeven ELG, Buth J, Cuypers PW, van Sambeek MR, Balm R, et al. A randomized trial comparing conventional and endovascular repair of abdominal aortic aneurysms. N Engl J Med. 2004;351:1607–18. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
