

High risk clinical characteristics for subarachnoid haemorrhage in patients with acute headache: prospective cohort study
- PMID: 21030443
- PMCID: PMC2966872
- DOI: 10.1136/bmj.c5204
High risk clinical characteristics for subarachnoid haemorrhage in patients with acute headache: prospective cohort study
Abstract
Objective: To identify high risk clinical characteristics for subarachnoid haemorrhage in neurologically intact patients with headache.
Design: Multicentre prospective cohort study over five years.
Setting: Six university affiliated tertiary care teaching hospitals in Canada. Data collected from November 2000 until November 2005.
Participants: Neurologically intact adults with a non-traumatic headache peaking within an hour.
Main outcome measures: Subarachnoid haemorrhage, as defined by any of subarachnoid haemorrhage on computed tomography of the head, xanthochromia in the cerebrospinal fluid, or red blood cells in the final sample of cerebrospinal fluid with positive results on angiography. Physicians completed data collection forms before investigations.
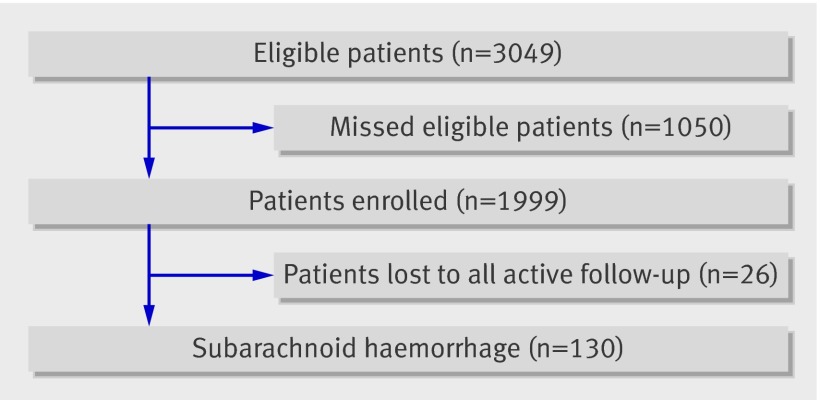
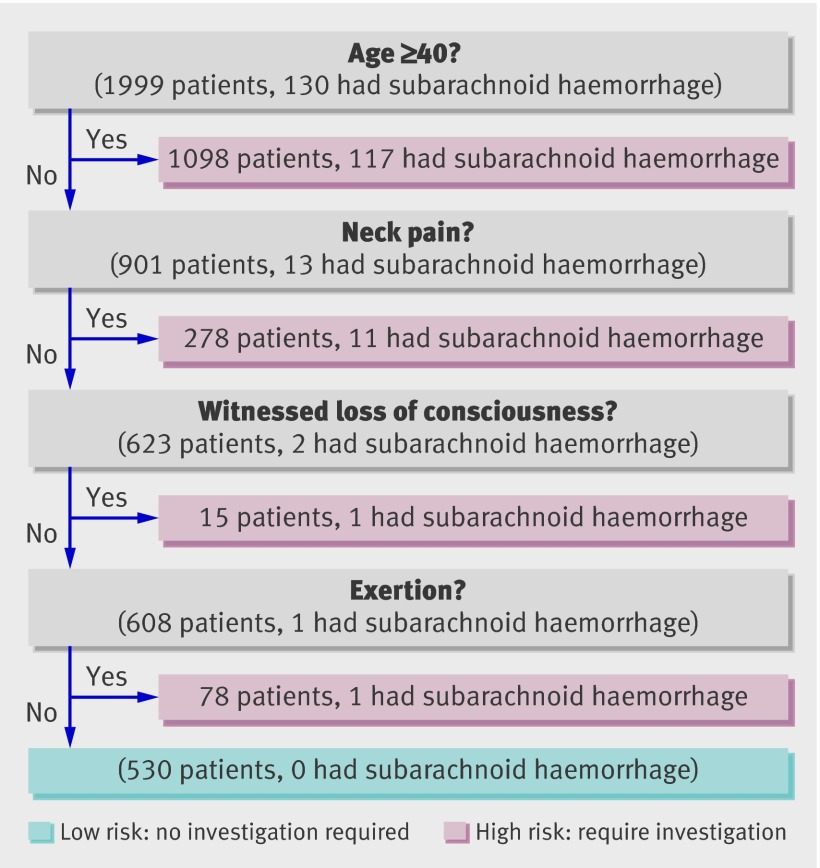
Results: In the 1999 patients enrolled there were 130 cases of subarachnoid haemorrhage. Mean (range) age was 43.4 (16-93), 1207 (60.4%) were women, and 1546 (78.5%) reported that it was the worst headache of their life. Thirteen of the variables collected on history and three on examination were reliable and associated with subarachnoid haemorrhage. We used recursive partitioning with different combinations of these variables to create three clinical decisions rules. All had 100% (95% confidence interval 97.1% to 100.0%) sensitivity with specificities from 28.4% to 38.8%. Use of any one of these rules would have lowered rates of investigation (computed tomography, lumbar puncture, or both) from the current 82.9% to between 63.7% and 73.5%.
Conclusion: Clinical characteristics can be predictive for subarachnoid haemorrhage. Practical and sensitive clinical decision rules can be used in patients with a headache peaking within an hour. Further study of these proposed decision rules, including prospective validation, could allow clinicians to be more selective and accurate when investigating patients with headache.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
Comment in
-
Decision rules in diagnosing subarachnoid haemorrhage.BMJ. 2010 Oct 28;341:c5586. doi: 10.1136/bmj.c5586. BMJ. 2010. PMID: 21030444 No abstract available.
-
Subarachnoid haemorrhage. Beware adopting rigid rules.BMJ. 2010 Dec 30;341:c7398. doi: 10.1136/bmj.c7398. BMJ. 2010. PMID: 21193503 No abstract available.
-
Subarachnoid haemorrhage. Cases may have been missed.BMJ. 2010 Dec 30;341:c7406. doi: 10.1136/bmj.c7406. BMJ. 2010. PMID: 21193506 No abstract available.
-
Subarachnoid haemorrhage. Reinventing the wheel, square.BMJ. 2010 Dec 30;341:c7414. doi: 10.1136/bmj.c7414. BMJ. 2010. PMID: 21193509 No abstract available.
-
[Can subarachnoid haemorrhage be recognised based on clinical characteristics?].Ned Tijdschr Geneeskd. 2011;155:A3145. Ned Tijdschr Geneeskd. 2011. PMID: 21527055 Dutch.
References
-
- Edlow JA, Panagos PD, Godwin SA, Thomas TL, Decker WW. Clinical policy: critical issues in the evaluation and management of adult patients presenting to the emergency department with acute headache. Ann Emerg Med 2008;52:407-36. - PubMed
-
- Perry JJ, Stiell IG, Wells GA, Spacek AM. Historical cohort study. Use and yield of investigations for alert patients with possible subarachnoid hemorrhage. Can J Emerg Med 2002;4:333-7. - PubMed
-
- Morgenstern LB, Huber JC, Luna-Gonzales H, Saldin KR, Grotta JC, Shaw SG, et al. Headache in the emergency department. Headache 2001;41:537-41. - PubMed
-
- Van Gijn J, Kerr RS, Rinkel GJ. Subarachnoid haemorrhage. Lancet 2007;369:306-18. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical