The learning curve for holmium laser enucleation of the prostate: a single-center experience
- PMID: 21031088
- PMCID: PMC2963781
- DOI: 10.4111/kju.2010.51.10.688
The learning curve for holmium laser enucleation of the prostate: a single-center experience
Abstract
Purpose: Holmium laser enucleation of the prostate (HoLEP) is known to have a steep learning curve and, as a result, its clinical usage has limitations. The purpose of this study was to analyze the learning curve and early complications following the HoLEP procedure.
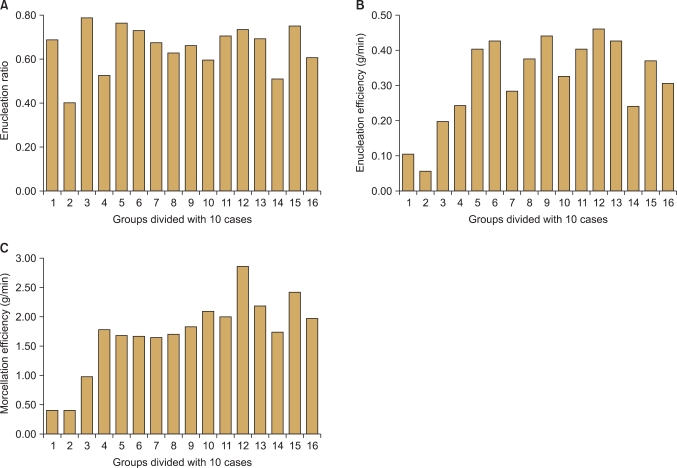
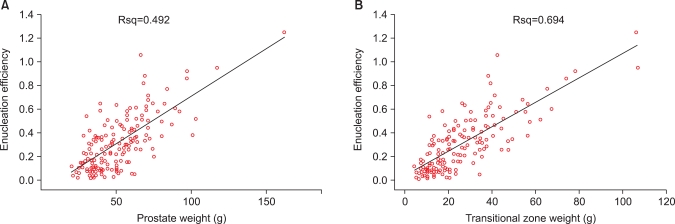
Materials and methods: A retrospective analysis was performed on 161 patients who had undergone the HoLEP procedure for lower urinary tract symptoms suggestive of benign prostatic hyperplasia (BPH) from July 2008 to September 2009. The procedure was done by two surgeons. Perioperatively, enucleated tissue weight, enucleation time, morcellation time, enucleation ratio (enucleation weight/transitional zone volume), and enucleation efficiency (enucleated weight/enucleation time) were analyzed, and early complications were assessed.
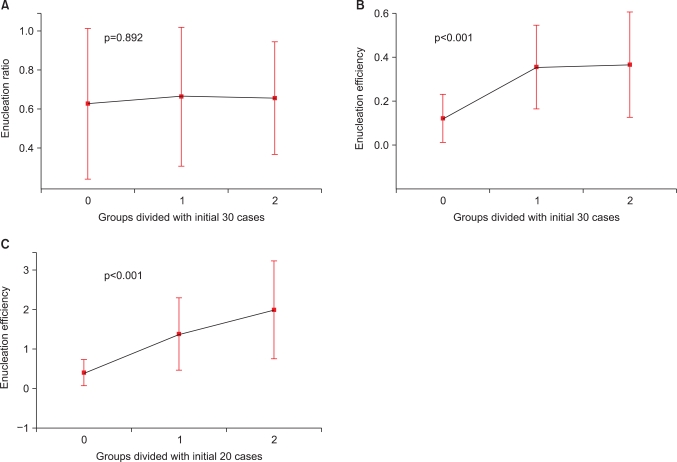
Results: Mean enucleation time, morcellation time, and enucleation ratio were 61.3 min (range, 10-180 min), 12.3 min (range, 2-60 min), and 0.66 (range, 0.07-2.51), respectively. In terms of efficiency, enucleation efficiency was 0.32 g/min (range, 0.02-1.25 g/min) and morcellation efficiency was 1.73 g/min (range, 0.1-7.7 g/min). Concerning the learning curve, enucleation efficiency was stationary after 30 cases (p<0.001), morcellation efficiency reached a learning curve at 20 cases (p=0.032), and enucleation ratio had no learning curve in this study. There were several cases of surgery-related complications, including bladder mucosal injury by the morcellator (13%), capsular injury during enucleation (7%), and conversion to a conventional resectoscopy procedure (15%), which showed a reduction in incidence with time.
Conclusions: The learning curve of HoLEP is steep; however, it can be overcome gradually. Further study is necessary with respect to long-term postoperative follow-up.
Keywords: Holmium; Lasers; Learning; Prostate; Prostatic hyperplasia.
Conflict of interest statement
The authors have nothing to disclose.
Figures
References
-
- Chilton CP, Mundy IP, Wiseman O. Results of holmium laser resection of the prostate for benign prostatic hyperplasia. J Endourol. 2000;14:533–534. - PubMed
-
- Moody JA, Lingeman JE. Holmium laser enucleation for prostate adenoma greater than 100 gm: comparison to open prostatectomy. J Urol. 2001;165:459–462. - PubMed
-
- Westenberg A, Gilling P, Kennett K, Frampton C, Fraundorfer M. Holmium laser resection of the prostate versus transurethral resection of the prostate: results of a randomized trial with 4-year minimum long-term followup. J Urol. 2004;172:616–619. - PubMed
-
- Montorsi F, Naspro R, Salonia A, Suardi N, Briganti A, Zanoni M, et al. Holmium laser enucleation versus transurethral resection of the prostate: results from a 2-center, prospective, randomized trial in patients with obstructive benign prostatic hyperplasia. J Urol. 2004;172:1926–1929. - PubMed
-
- Kuntz RM, Lehrich K. Transurethral holmium laser enucleation versus transvesical open enucleation for prostate adenoma greater than 100 gm: a randomized prospective trial of 120 patients. J Urol. 2002;168:1465–1469. - PubMed
LinkOut - more resources
Full Text Sources