

Long-acting beta-agonists in the management of chronic obstructive pulmonary disease: current and future agents
- PMID: 21034447
- PMCID: PMC2991288
- DOI: 10.1186/1465-9921-11-149
Long-acting beta-agonists in the management of chronic obstructive pulmonary disease: current and future agents
Abstract
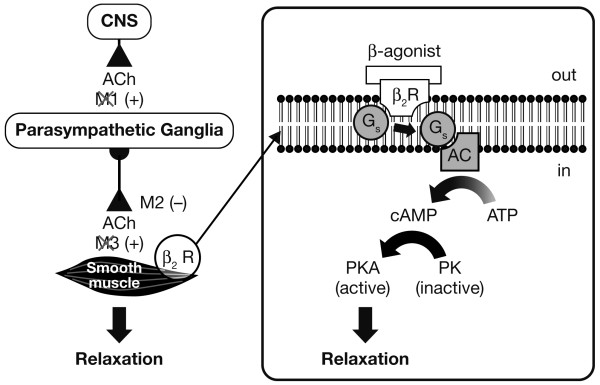
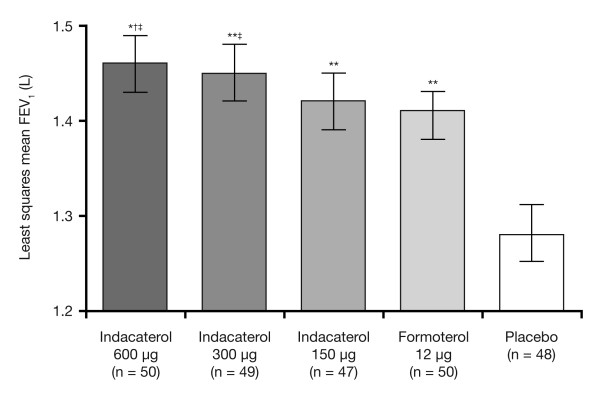
Chronic obstructive pulmonary disease (COPD) is characterized by progressive airflow limitation and debilitating symptoms. For patients with moderate-to-severe COPD, long-acting bronchodilators are the mainstay of therapy; as symptoms progress, guidelines recommend combining bronchodilators from different classes to improve efficacy. Inhaled long-acting β2-agonists (LABAs) have been licensed for the treatment of COPD since the late 1990s and include formoterol and salmeterol. They improve lung function, symptoms of breathlessness and exercise limitation, health-related quality of life, and may reduce the rate of exacerbations, although not all patients achieve clinically meaningful improvements in symptoms or health related quality of life. In addition, LABAs have an acceptable safety profile, and are not associated with an increased risk of respiratory mortality, although adverse effects such as palpitations and tremor may limit the dose that can be tolerated. Formoterol and salmeterol have 12-hour durations of action; however, sustained bronchodilation is desirable in COPD. A LABA with a 24-hour duration of action could provide improvements in efficacy, compared with twice-daily LABAs, and the once-daily dosing regimen could help improve compliance. It is also desirable that a new LABA should demonstrate fast onset of action, and a safety profile at least comparable to existing LABAs.A number of novel LABAs with once-daily profiles are in development which may be judged against these criteria. Indacaterol, a LABA with a 24-hour duration of bronchodilation and fast onset of action, is the most advanced of these. Preliminary results from large clinical trials suggest indacaterol improves lung function compared with placebo and other long-acting bronchodilators. Other LABAs with a 24-hour duration of bronchodilation include carmoterol, vilanterol trifenatate and oldaterol, with early results indicating potential for once-daily dosing in humans.The introduction of once-daily LABAs also provides the opportunity to develop combination inhalers of two or more classes of once-daily long-acting bronchodilators, which may be advantageous for COPD patients through simplification of treatment regimens as well as improvements in efficacy. Once-daily LABAs used both alone and in combination with long-acting muscarinic antagonists represent a promising advance in the treatment of COPD, and are likely to further improve outcomes for patients.
Figures
References
-
- Global Initiative for Chronic Obstructive Lung Disease (GOLD) Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. 2009.
-
- National Institute for Health and Clinical Excellence. Chronic obstructive pulmonary disease: Management of chronic obstructive pulmonary disease in adults in primary and secondary care. National Clinical Guideline Centre; 2010. http://guidance.nice.org.uk/CG101/Guidance/pdf/English Accessed June 28, 2010.
-
- Hasegawa M, Makita H, Nasuhara Y, Odajima N, Nagai K, Ito Y, Betsuyaku T, Nishimura M. Relationship between improved airflow limitation and changes in airway caliber induced by inhaled anticholinergics in chronic obstructive pulmonary disease. Thorax. 2009;64:332–8. doi: 10.1136/thx.2008.103671. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
