

Central venous O₂ saturation and venous-to-arterial CO₂ difference as complementary tools for goal-directed therapy during high-risk surgery
- PMID: 21034476
- PMCID: PMC3219300
- DOI: 10.1186/cc9310
Central venous O₂ saturation and venous-to-arterial CO₂ difference as complementary tools for goal-directed therapy during high-risk surgery
Abstract
Introduction: Central venous oxygen saturation (ScvO2) is a useful therapeutic target in septic shock and high-risk surgery. We tested the hypothesis that central venous-to-arterial carbon dioxide difference (P(cv-a)CO2), a global index of tissue perfusion, could be used as a complementary tool to ScvO2 for goal-directed fluid therapy (GDT) to identify persistent low flow after optimization of preload has been achieved by fluid loading during high-risk surgery.
Methods: This is a secondary analysis of results obtained in a study involving 70 adult patients (ASA I to III), undergoing major abdominal surgery, and treated with an individualized goal-directed fluid replacement therapy. All patients were managed to maintain a respiratory variation in peak aortic flow velocity below 13%. Cardiac index (CI), oxygen delivery index (DO2i), ScvO2, P(cv-a)CO2 and postoperative complications were recorded blindly for all patients.
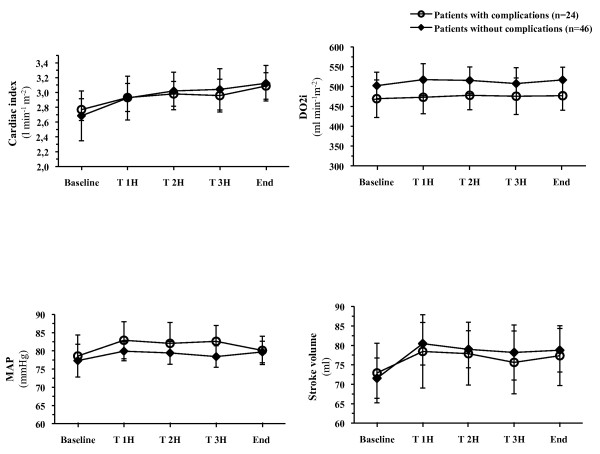
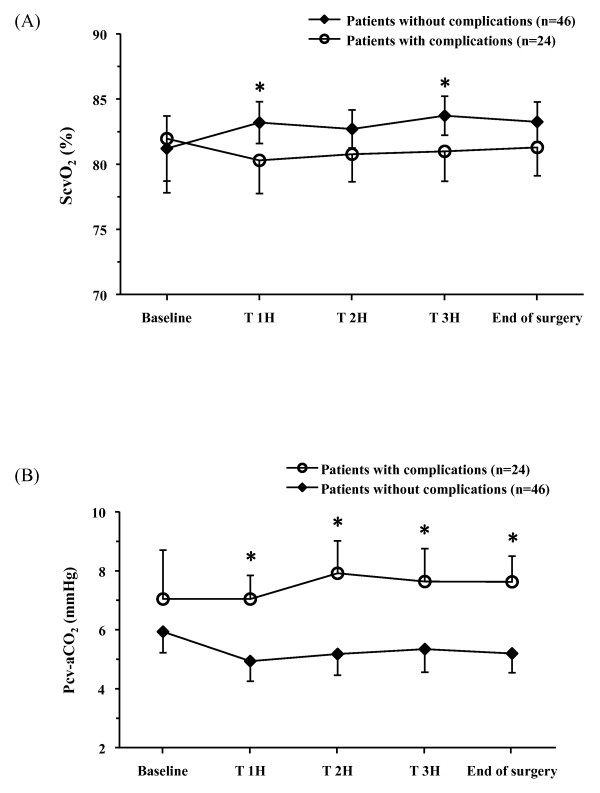
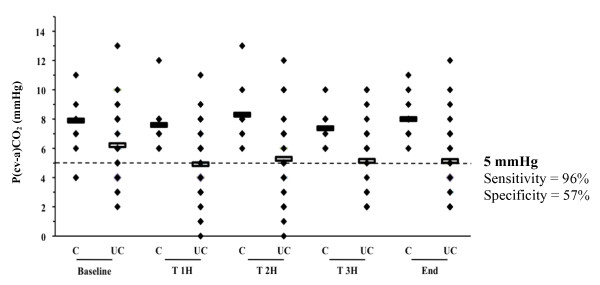
Results: A total of 34% of patients developed postoperative complications. At baseline, there was no difference in demographic or haemodynamic variables between patients who developed complications and those who did not. In patients with complications, during surgery, both mean ScvO2 (78 ± 4 versus 81 ± 4%, P = 0.017) and minimal ScvO2 (minScvO2) (67 ± 6 versus 72 ± 6%, P = 0.0017) were lower than in patients without complications, despite perfusion of similar volumes of fluids and comparable CI and DO2i values. The optimal ScvO2 cut-off value was 70.6% and minScvO2 < 70% was independently associated with the development of postoperative complications (OR = 4.2 (95% CI: 1.1 to 14.4), P = 0.025). P(cv-a)CO2 was larger in patients with complications (7.8 ± 2 versus 5.6 ± 2 mmHg, P < 10-6). In patients with complications and ScvO2 ≥ 71%, P(cv-a)CO2 was also significantly larger (7.7 ± 2 versus 5.5 ± 2 mmHg, P < 10-6) than in patients without complications. The area under the receiver operating characteristic (ROC) curve was 0.785 (95% CI: 0.74 to 0.83) for discrimination of patients with ScvO2 ≥ 71% who did and did not develop complications, with 5 mmHg as the most predictive threshold value.
Conclusions: ScvO2 reflects important changes in O2 delivery in relation to O2 needs during the perioperative period. A P(cv-a)CO2 < 5 mmHg might serve as a complementary target to ScvO2 during GDT to identify persistent inadequacy of the circulatory response in face of metabolic requirements when an ScvO2 ≥ 71% is achieved.
Trial registration: Clinicaltrials.gov Identifier: NCT00852449.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
