

YKL-40: a novel prognostic fluid biomarker for preclinical Alzheimer's disease
- PMID: 21035623
- PMCID: PMC3011944
- DOI: 10.1016/j.biopsych.2010.08.025
YKL-40: a novel prognostic fluid biomarker for preclinical Alzheimer's disease
Erratum in
- Biol Psychiatry. 2011 Feb 15;69(4):389
Abstract
Background: Disease-modifying therapies for Alzheimer's disease (AD) would be most effective during the preclinical stage (pathology present, cognition intact) before significant neuronal loss occurs. Therefore, biomarkers that detect AD pathology in its early stages and predict dementia onset and progression will be invaluable for patient care and efficient clinical trial design.
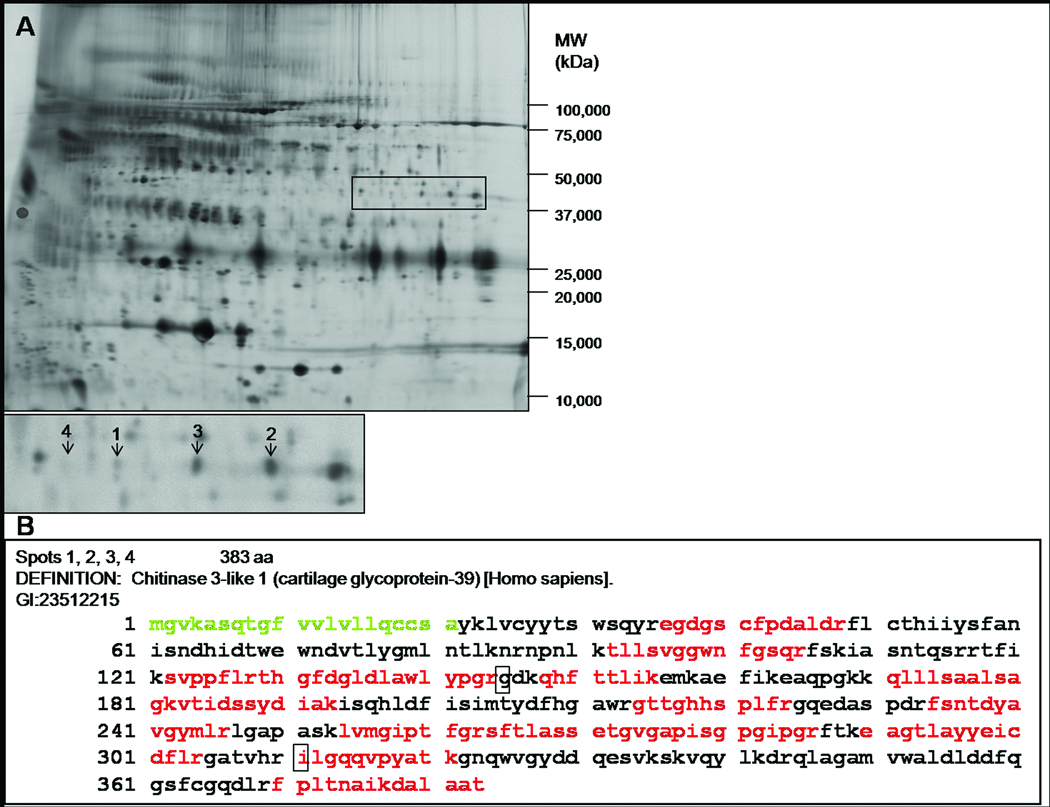
Methods: AD-associated changes in cerebrospinal fluid (CSF) were measured using two-dimensional difference gel electrophoresis and liquid chromatography tandem mass spectrometry. Subsequently, CSF YKL-40 was measured by enzyme-linked immunosorbent assay in the discovery cohort (n = 47), validation cohort (n = 292) with paired plasma samples (n = 237), frontotemporal lobar degeneration (n=9) [corrected], and progressive supranuclear palsy (PSP; n = 6). Immunohistochemistry was performed to identify source(s) of YKL-40 in human AD brain.
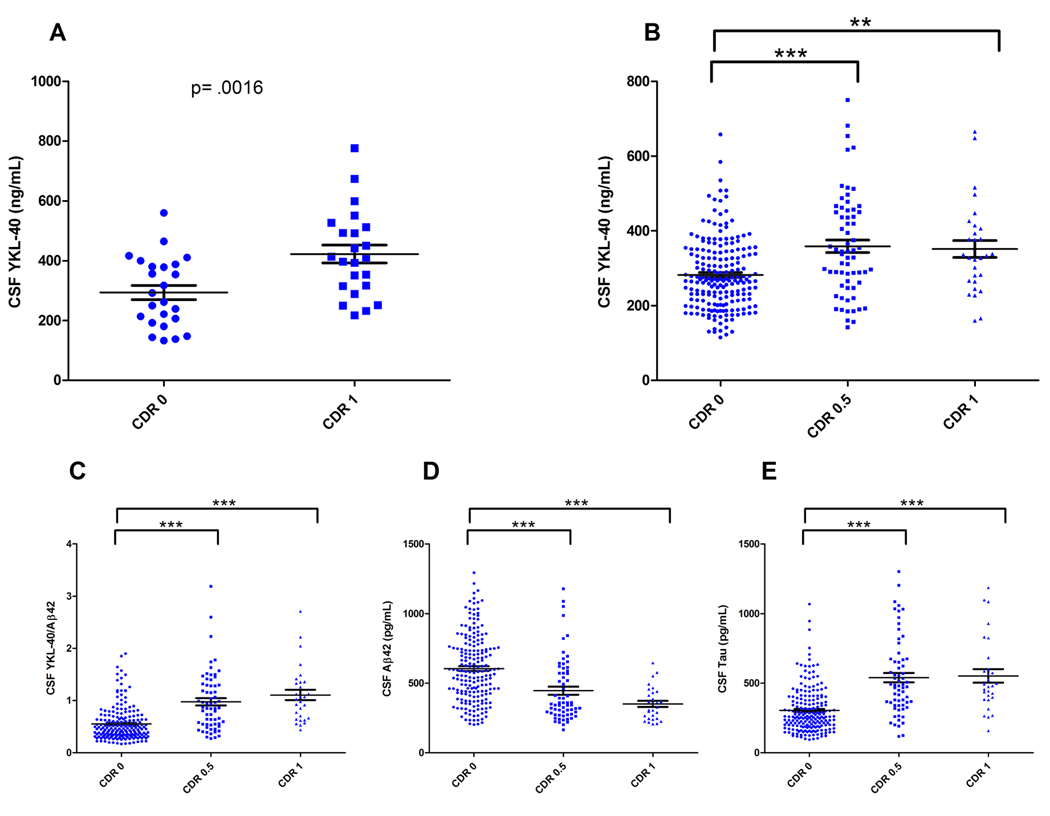
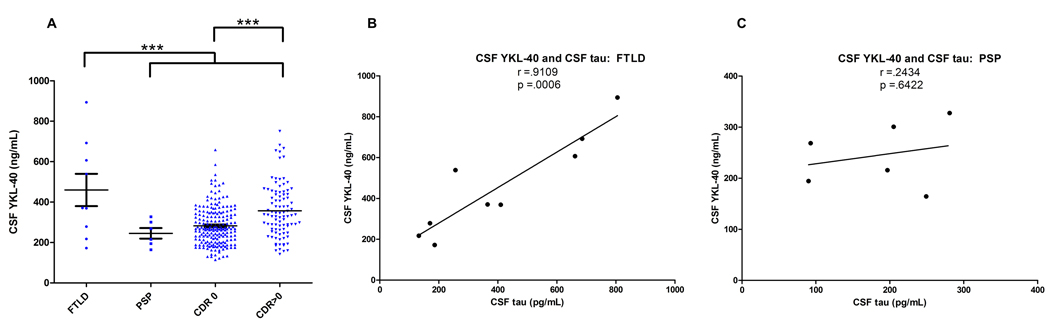
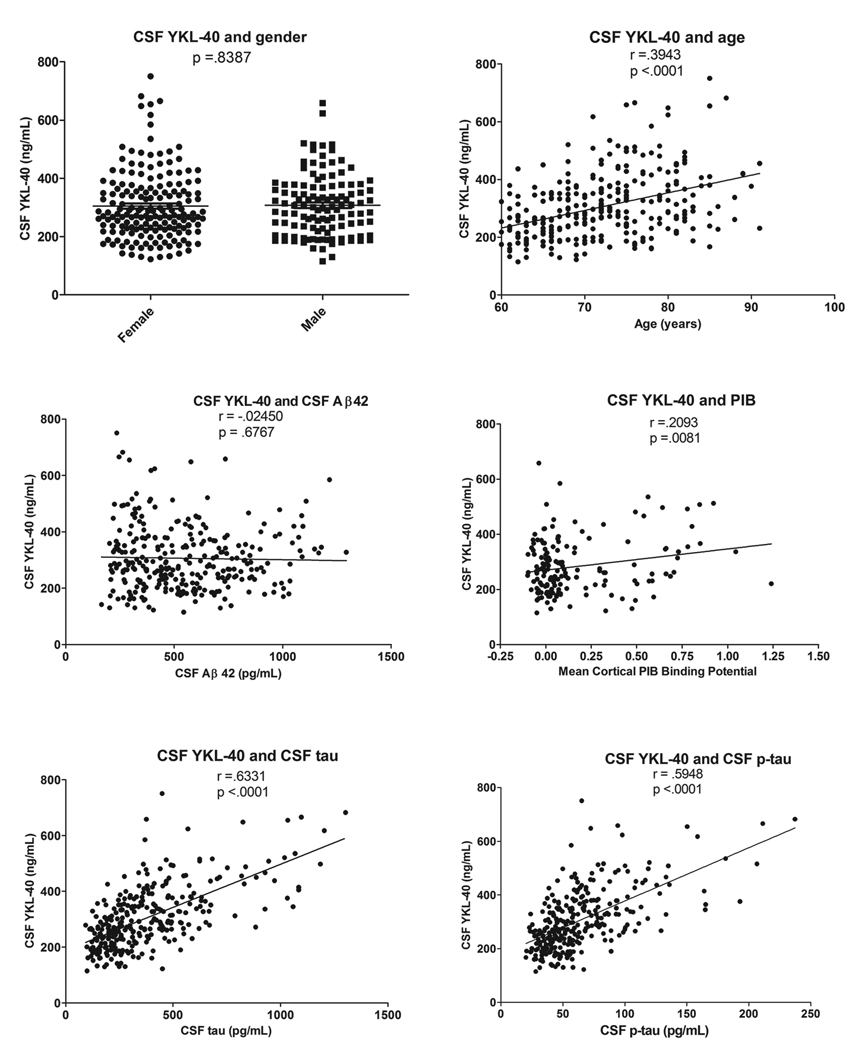
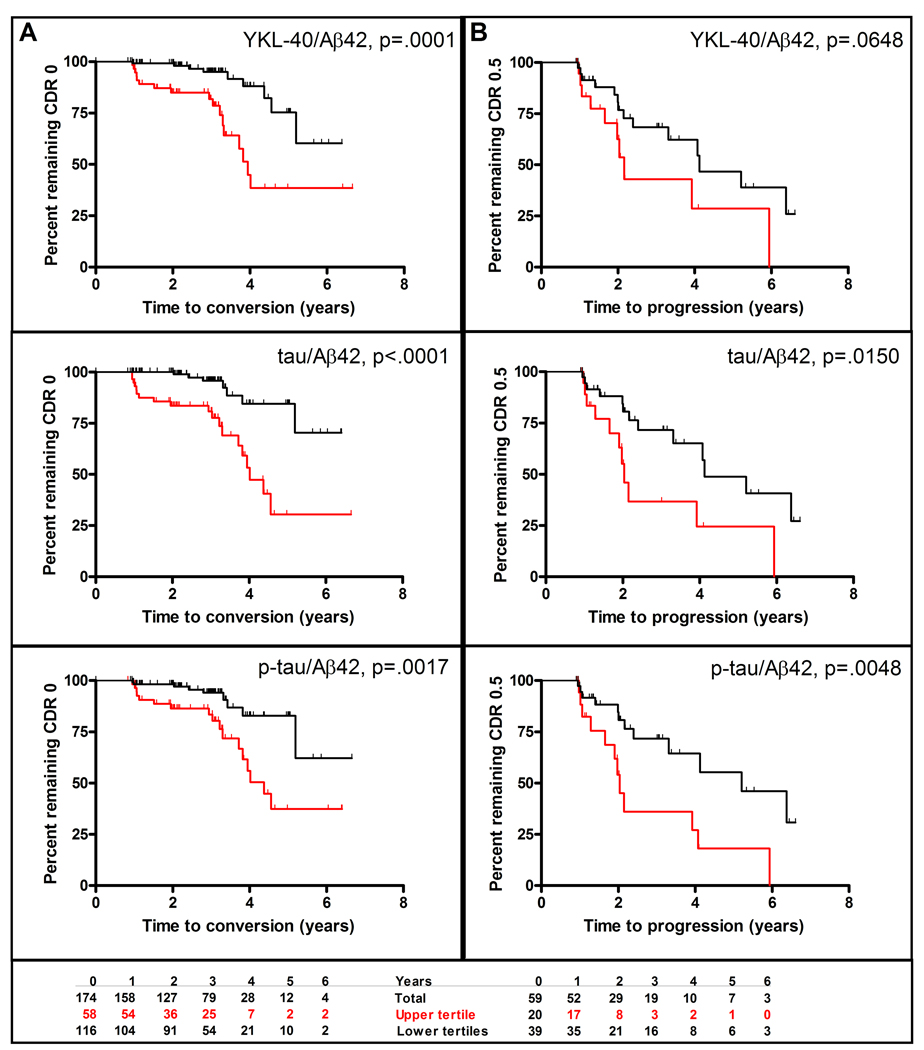
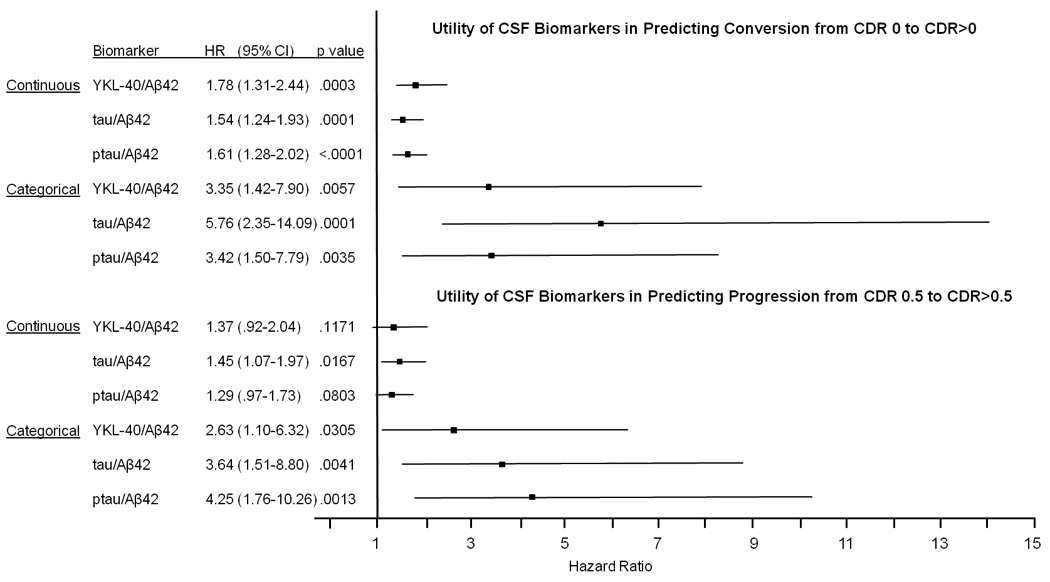
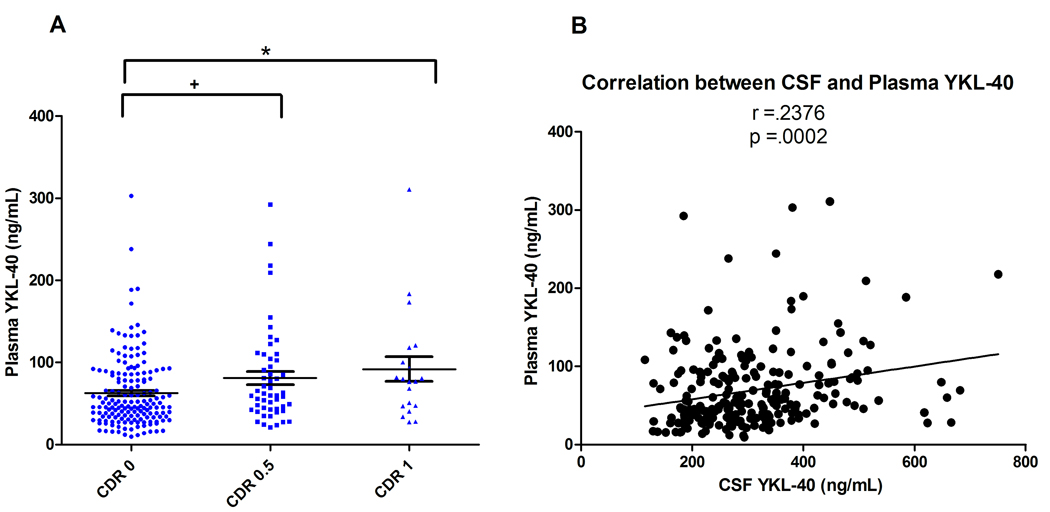
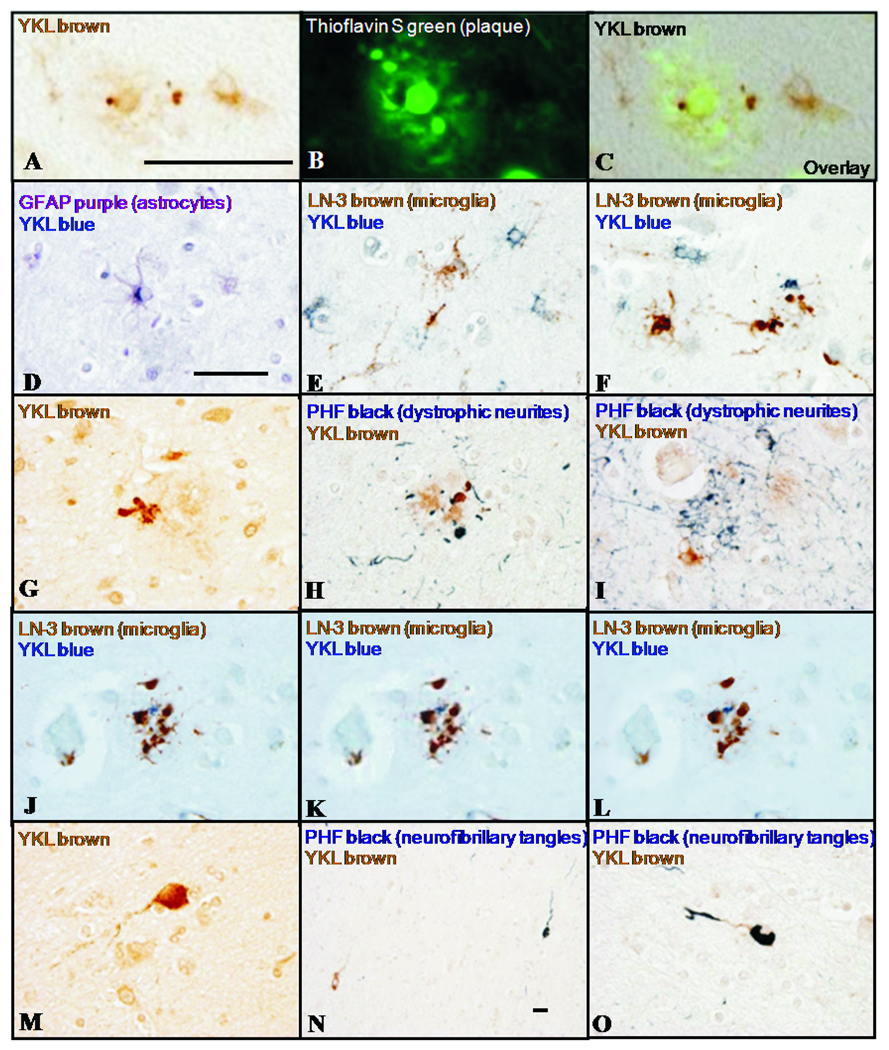
Results: Discovery and validation cohorts, showed higher mean CSF YKL-40 in very mild and mild AD-type dementia (Clinical Dementia Rating [CDR] 0.5 and 1) versus control subjects (CDR 0) and PSP subjects. Importantly, CSF YKL-40/Aβ42 ratio predicted risk of developing cognitive impairment (CDR 0 to CDR > 0 conversion), as well as the best CSF biomarkers identified to date, tau/Aβ42 and p-tau 181/Aβ42. Mean plasma YKL-40 was higher in CDR 0.5 and 1 versus CDR 0, and correlated with CSF levels. YKL-40 immunoreactivity labeled astrocytes near a subset of amyloid plaques, implicating YKL-40 in the neuroinflammatory response to Aβ deposition.
Conclusions: These data demonstrate that YKL-40, a putative indicator of neuroinflammation, is elevated in AD and, together with Aβ42, has potential prognostic utility as a biomarker for preclinical AD.
Copyright © 2010 Society of Biological Psychiatry. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Davies L, Wolska B, Hilbich C, Multhaup G, Martins R, Simms G, et al. A4 amyloid protein deposition and the diagnosis of Alzheimer's disease: prevalence in aged brains determined by immunocytochemistry compared with conventional neuropathologic techniques. Neurology. 1988;38:1688–1693. - PubMed
-
- Morris J, Price J. Pathologic correlates of nondemented aging, mild cognitive impairment, and early stage Alzheimer's disease. J Mol Neurosci. 2001;17:101–118. - PubMed
-
- Hulette CM, Welsh-Bohmer KA, Murray MG, Saunders AM, Mash DC, McIntyre LM. Neuropathological and neuropsychological changes in "normal" aging: Evidence for preclinical Alzheimer disease in cognitively normal individuals. J Neuropathol Exp Neurol. 1998;57:1168–1174. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 AG031278/AG/NIA NIH HHS/United States
- P01 AG026276/AG/NIA NIH HHS/United States
- P50 AG005136/AG/NIA NIH HHS/United States
- T32 NS007205/NS/NINDS NIH HHS/United States
- K23 AG031861/AG/NIA NIH HHS/United States
- UL1 TR000448/TR/NCATS NIH HHS/United States
- P41 RR000954/RR/NCRR NIH HHS/United States
- K23-AG031861/AG/NIA NIH HHS/United States
- P30 NS057105/NS/NINDS NIH HHS/United States
- P50 AG05681/AG/NIA NIH HHS/United States
- P50 AG023501/AG/NIA NIH HHS/United States
- U01 AG016976/AG/NIA NIH HHS/United States
- P01 AG003991/AG/NIA NIH HHS/United States
- R01AG031278/AG/NIA NIH HHS/United States
- P50 AG005681/AG/NIA NIH HHS/United States
- P01 AG03991/AG/NIA NIH HHS/United States
- UL1 RR024992/RR/NCRR NIH HHS/United States
- P01 AG019724/AG/NIA NIH HHS/United States
- U01 AG16976/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
