

Axial length measurements by contact and immersion techniques in pediatric eyes with cataract
- PMID: 21035871
- PMCID: PMC3052929
- DOI: 10.1016/j.ophtha.2010.06.042
Axial length measurements by contact and immersion techniques in pediatric eyes with cataract
Abstract
Purpose: To compare axial length measurements by contact and immersion techniques in pediatric cataractous eyes.
Design: Prospective, comparative case series.
Participants: In this prospective study, 50 cataractous eyes of 50 children were enrolled. In bilateral cataract, only 1 eye was selected to avoid a correlation effect in statistical analyses.
Methods: Axial length was measured by both contact and immersion techniques for all eyes, randomized as to which to perform first to avoid measurement bias.
Main outcome measures: Axial length measured by contact and immersion techniques and the difference between contact and immersion technique axial length measurements.
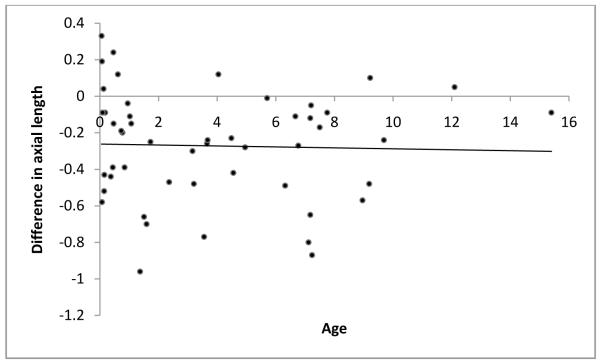
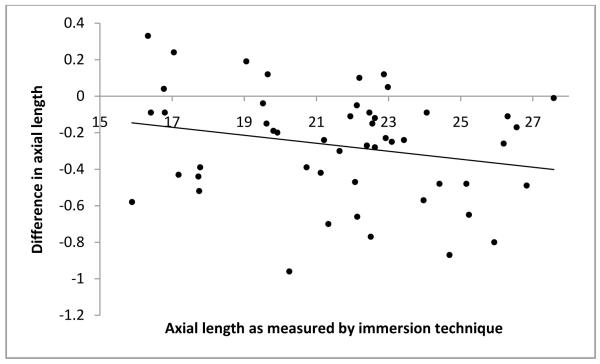
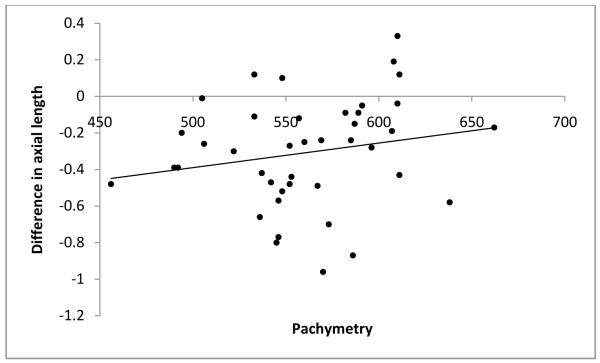
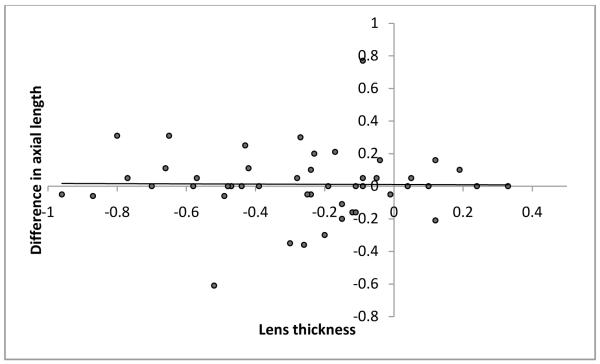
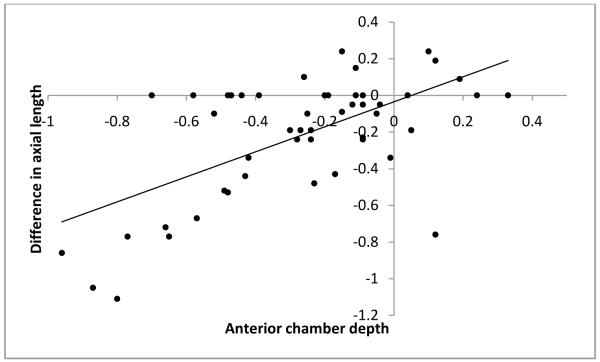
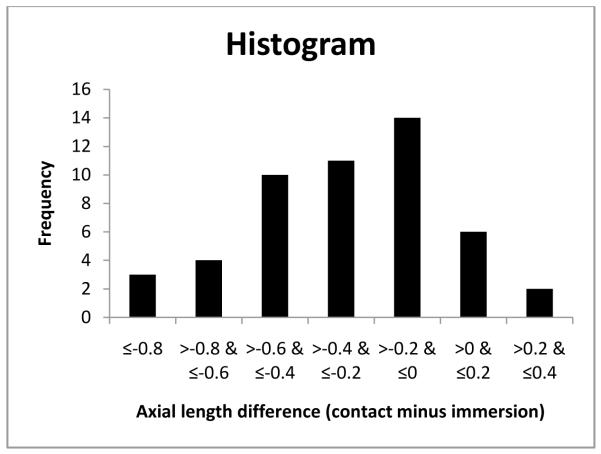
Results: Mean age±standard deviation at cataract surgery and at axial length measurement was 3.87±3.72 years. Axial length measurement by contact technique was significantly shorter as compared with immersion technique (21.36±3.04 mm and 21.63±3.09 mm, respectively; P<0.001). Axial length measurements using the contact technique were on an average 0.27 mm shorter than those obtained using the immersion technique. Forty-two eyes (84%) had shorter axial length when measured using the contact technique as compared with the immersion technique. Lens thickness measurement by contact technique was not significantly different from that of immersion technique (3.61±0.74 and 3.60±0.67 mm, respectively; P = 0.673). Anterior chamber depth measurement was significantly more shallow with the contact technique (3.39±0.59 mm and 3.69±0.54 mm, respectively; P<0.001). Intraocular lens power needed for emmetropia was significantly different (28.68 diopters [D] vs. 27.63 D; P<0.001).
Conclusions: Contact A-scan measurements yielded shorter axial length than immersion A-scan measurements. This difference was mainly the result of the anterior chamber depth rather than the lens thickness value. During intraocular lens (IOL) power calculation, if axial length measured by contact technique is used, it will result in the use of an average 1-D stronger IOL power than is actually required. This can lead to induced myopia in the postoperative refraction.
Copyright © 2011 American Academy of Ophthalmology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Wilson ME, Jr, Bartholomew LR, Trivedi RH. Pediatric cataract surgery and intraocular lens implantation: practice styles and preferences of the 2001 ASCRS and AAPOS memberships. J Cataract Refract Surg. 2003;29:1811–20. - PubMed
-
- Trivedi RH, Peterseim MM, Wilson ME., Jr New techniques and technologies for pediatric cataract surgery. Curr Opin Ophthalmol. 2005;16:289–93. - PubMed
-
- Moore DB, Ben Zion I, Neely DE, et al. Accuracy of biometry in pediatric cataract extraction with primary intraocular lens implantation. J Cataract Refract Surg. 2008;34:1940–7. - PubMed
-
- Crouch ER, Crouch ER, Jr, Pressman SH. Prospective analysis of pediatric pseudophakia: myopic shift and postoperative outcomes. J AAPOS. 2002;6:277–82. - PubMed
-
- Plager DA, Lipsky SN, Snyder SK, et al. Capsular management and refractive error in pediatric intraocular lenses. Ophthalmology. 1997;104:600–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
