

Human papillomavirus 16-associated cervical intraepithelial neoplasia in humans excludes CD8 T cells from dysplastic epithelium
- PMID: 21037100
- PMCID: PMC3075978
- DOI: 10.4049/jimmunol.1002756
Human papillomavirus 16-associated cervical intraepithelial neoplasia in humans excludes CD8 T cells from dysplastic epithelium
Abstract
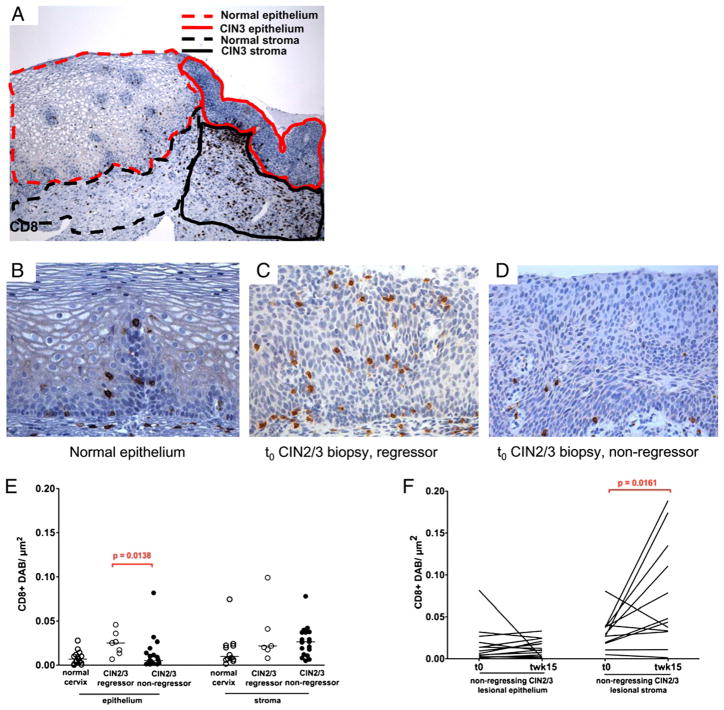
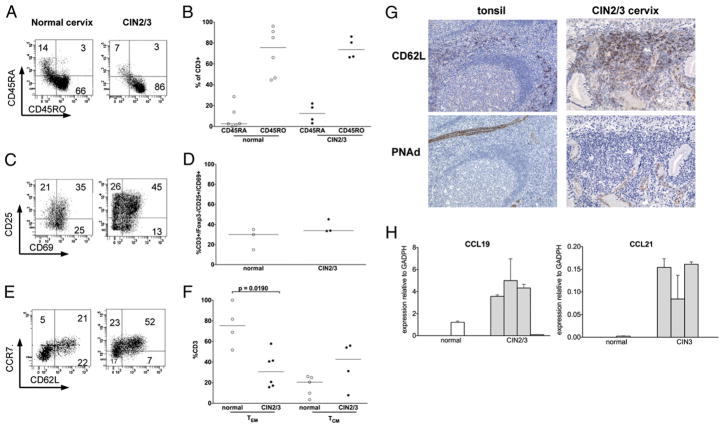
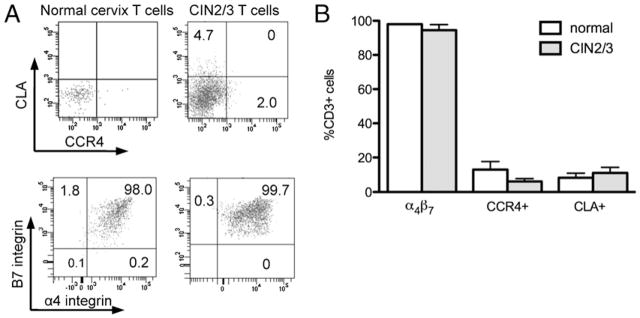
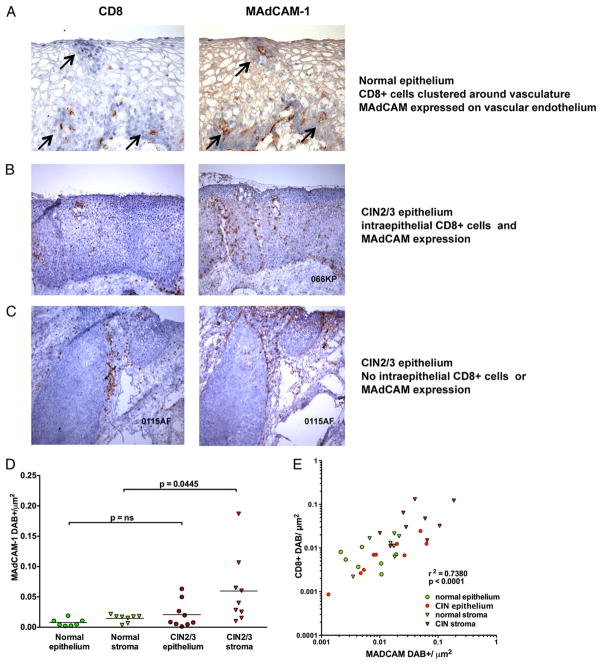
High-grade cervical dysplasia caused by human papillomavirus (HPV) type 16 is a lesion that should be susceptible to an HPV-specific immune response; disease initiation and persistence is predicated on expression of two viral Ags, E6 and E7. In immune-competent subjects, at least 25% of HPV16(+) high-grade cervical dysplasia lesions undergo complete regression. However, in the peripheral blood, naturally occurring IFN-γ T cell responses to HPV E6 and E7 are weak, requiring ex vivo sensitization to detect, and are not sufficiently sensitive to predict regression. In this study, we present immunologic data directly assessing cervical lymphocytes from this cohort. We found that nearly all cervical tissue T cells express the mucosal homing receptor, α(4)β(7) surface integrin. T cells isolated from dysplastic mucosa were skewed toward a central memory phenotype compared with normal mucosal resident T cells, and dysplastic lesions expressed transcripts for CCL19 and CCL21, raising the possibility that the tissue itself sustains a response that is not detectable in the blood. Moreover, lesion regression in the study window could retrospectively be predicted at study entry by the ability of CD8(+) T cells to gain access to lesional epithelium. Vascular endothelial expression of mucosal addressin cell adhesion molecule-1, the ligand that supports entry of α(4)β(7)(+) T cells into tissues, colocalized tightly with the distribution of CD8 T cells and was not expressed in persistent dysplastic epithelium. These findings suggest that dysregulated expression of vascular adhesion molecules plays a role in immune evasion very early in the course of HPV disease.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Frazer IH, Lowy DR, Schiller JT. Prevention of cancer through immunization: Prospects and challenges for the 21st century. Eur J Immunol. 2007;37(Suppl 1):S148–S155. - PubMed
-
- Bosch FX, Manos MM, Muñoz N, Sherman M, Jansen AM, Peto J, Schiffman MH, Moreno V, Kurman R, Shah KV. Prevalence of human papillomavirus in cervical cancer: a worldwide perspective. International biological study on cervical cancer (IBSCC) Study Group. J Natl Cancer Inst. 1995;87:796–802. - PubMed
-
- Fleurence RL, Dixon JM, Milanova TF, Beusterien KM. Review of the economic and quality-of-life burden of cervical human papillomavirus disease. Am J Obstet Gynecol. 2007;196:206–212. - PubMed
-
- Monk BJ, Herzog TJ. The evolution of cost-effective screening and prevention of cervical carcinoma: implications of the 2006 consensus guidelines and human papillomavirus vaccination. Am J Obstet Gynecol. 2007;197:337–339. - PubMed
-
- Insinga RP, Glass AG, Rush BB. The health care costs of cervical human papillomavirus—related disease. Am J Obstet Gynecol. 2004;191:114–120. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
