

Pediatric brain tumor treatment: growth consequences and their management
- PMID: 21037539
- PMCID: PMC4148717
Pediatric brain tumor treatment: growth consequences and their management
Abstract
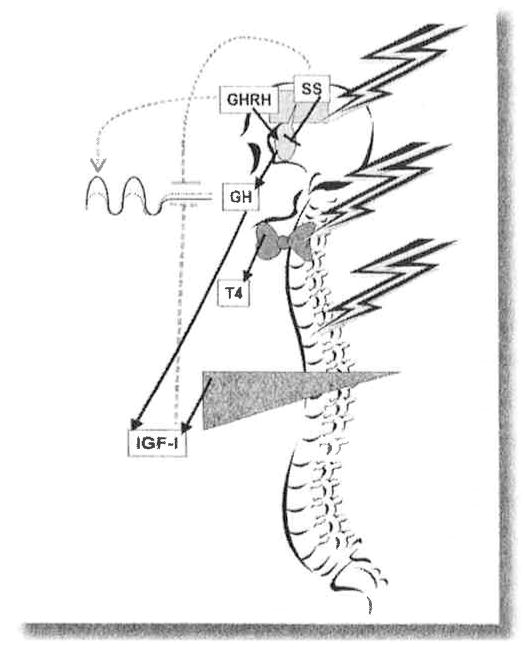
Tumors of the central nervous system, the most common solid tumors of childhood, are a major source of cancer-related morbidity and mortality in children. Survival rates have improved significantly following treatment for childhood brain tumors, with this growing cohort of survivors at high risk of adverse medical and late effects. Endocrine morbidities are the most prominent disorder among the spectrum of longterm conditions, with growth hormone deficiency the most common endocrinopathy noted, either from tumor location or after cranial irradiation and treatment effects on the hypothalamic/pituitary unit. Deficiency of other anterior pituitary hormones can contribute to negative effects on growth, body image and composition, sexual function, skeletal health, and quality of life. Pediatric and adult endocrinologists often provide medical care to this increasing population. Therefore, a thorough understanding of the epidemiology and pathophysiology of growth failure as a consequence of childhood brain tumor, both during and after treatment, is necessary and the main focus of this review.
Figures
References
-
- Packer RJ, MacDonald T, Vezina G. Central nervous system tumors. Pediatr Clin North Am. 2008;55(1):121–145. xi. - PubMed
-
- Bleyer WA. Epidemiologic impact of children with brain tumors. Childs Nerv Syst. 1999;15(11–12):758–763. - PubMed
-
- Weir HK, Thun MJ, Hankey BF, Ries LA, Howe HL, Wingo PA, Jemal A, Ward E, Anderson RN, Edwards BK. Annual report to the nation on the status of cancer, 1975–2000, featuring the uses of surveillance data for cancer prevention and control. J Natl Cancer Inst. 2003;95(17):1276–1299. - PubMed
-
- Sklar CA. Overview of the effects of cancer therapies: the nature, scale and breadth of the problem. Acta Paediatr. 1999;88(suppl 433):1–4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical