

Cerebral collateral circulation in carotid artery disease
- PMID: 21037845
- PMCID: PMC2842960
- DOI: 10.2174/157340309789317887
Cerebral collateral circulation in carotid artery disease
Abstract
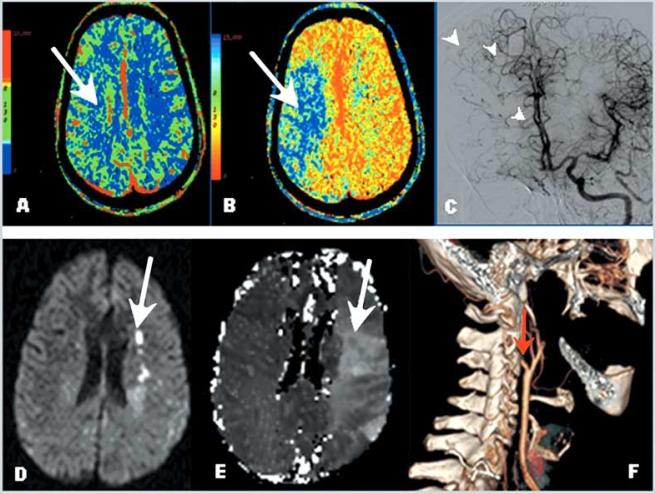
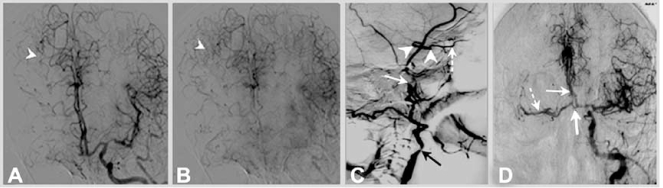
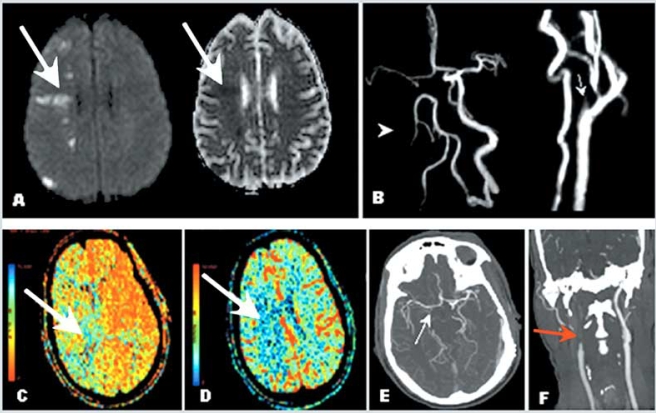
Carotid artery disease is common and increases the risk of stroke. However, there is wide variability on the severity of clinical manifestations of carotid disease, ranging from asymptomatic to fatal stroke. The collateral circulation has been recognized as an important aspect of cerebral circulation affecting the risk of stroke as well as other features of stroke presentation, such as stroke patterns in patients with carotid artery disease. The cerebral circulation attempts to maintain constant cerebral perfusion despite changes in systemic conditions, due to its ability to autoregulate blood flow. In case that one of the major cerebral arteries is compromised by occlusive disease, the cerebral collateral circulation plays an important role in preserving cerebral perfusion through enhanced recruitment of blood flow. With the advent of techniques that allow rapid evaluation of cerebral perfusion, the collateral circulation of the brain and its effectiveness may also be evaluated, allowing for prompt assessment of patients with acute stroke due to involvement of the carotid artery, and risk stratification of patients with carotid stenosis in chronic stages. Understanding the cerebral collateral circulation provides a basis for the future development of new diagnostic tools, risk stratification, predictive models and new therapeutic modalities. In the present review we discuss basic aspects of the cerebral collateral circulation, diagnostic methods to assess collateral circulation, and implications in occlusive carotid artery disease.
Keywords: Carotid artery disease; cerebral collateral circulation; cerebral perfusion; stroke..
Figures
References
-
- Barnett HJ, Taylor DW, Eliasziw M, et al. Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis. North american symptomatic carotid endarterectomy trial collaborators. N Engl J Med. 1998;339:1415–25. - PubMed
-
- Johnston SC, O'Meara ES, Manolio TA, et al. Cognitive impairment and decline are associated with carotid artery disease in patients without clinically evident cerebrovascular disease. Ann Intern Med. 2004;140:237–47. - PubMed
-
- van Oijen M, de Jong FJ, Witteman JC, et al. Atherosclerosis and risk for dementia. Ann Neurol. 2007;61:403–10. - PubMed
-
- Sacco RL. Clinical practice. Extracranial carotid stenosis. N Engl J Med. 2001;345:1113–8. - PubMed
-
- AbuRahma AF, Stone PA, Abu-Halimah S, Welch CA. Natural history of carotid artery occlusion contralateral to carotid endarterectomy. J Vasc Surg. 2006;44:62–66. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
