

Cost-consequence analysis of remifentanil-based analgo-sedation vs. conventional analgesia and sedation for patients on mechanical ventilation in the Netherlands
- PMID: 21040558
- PMCID: PMC3219979
- DOI: 10.1186/cc9313
Cost-consequence analysis of remifentanil-based analgo-sedation vs. conventional analgesia and sedation for patients on mechanical ventilation in the Netherlands
Abstract
Introduction: Hospitals are increasingly forced to consider the economics of technology use. We estimated the incremental cost-consequences of remifentanil-based analgo-sedation (RS) vs. conventional analgesia and sedation (CS) in patients requiring mechanical ventilation (MV) in the intensive care unit (ICU), using a modelling approach.
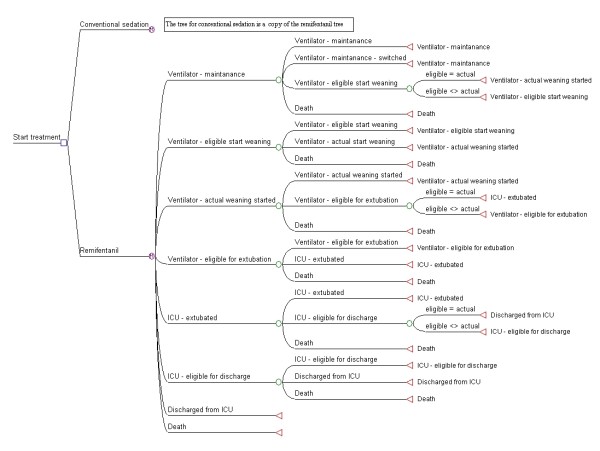
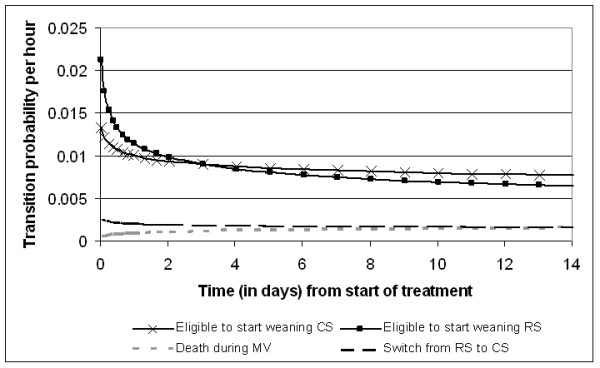
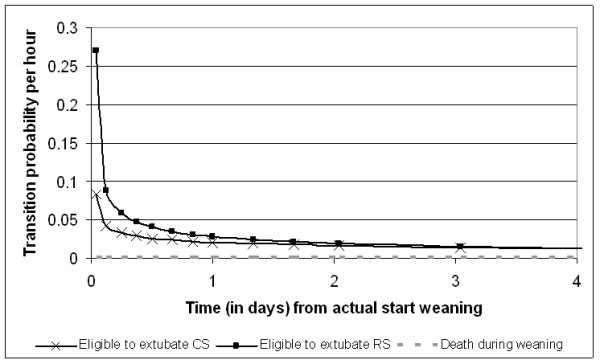
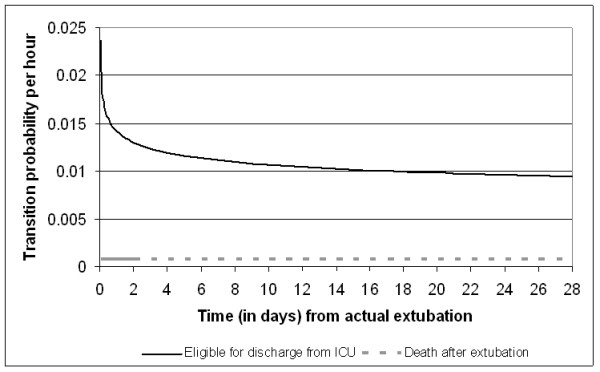
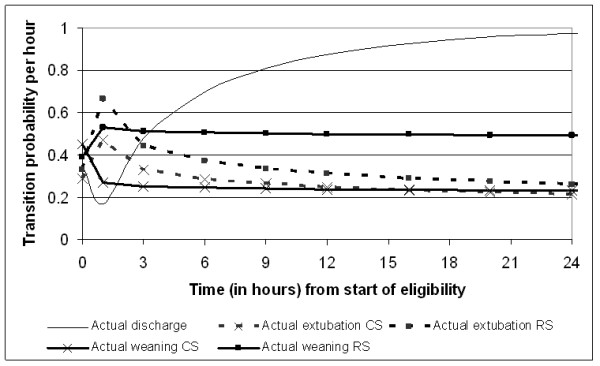
Methods: A Markov model was developed to describe patient flow in the ICU. The hourly probabilities to move from one state to another were derived from UltiSAFE, a Dutch clinical study involving ICU patients with an expected MV-time of two to three days requiring analgesia and sedation. Study medication was either: CS (morphine or fentanyl combined with propofol, midazolam or lorazepam) or: RS (remifentanil, combined with propofol when required). Study drug costs were derived from the trial, whereas all other ICU costs were estimated separately in a Dutch micro-costing study. All costs were measured from the hospital perspective (price level of 2006). Patients were followed in the model for 28 days. We also studied the sub-population where weaning had started within 72 hours.
Results: The average total 28-day costs were €15,626 with RS versus €17,100 with CS, meaning a difference in costs of €1474 (95% CI -2163, 5110). The average length-of-stay (LOS) in the ICU was 7.6 days in the RS group versus 8.5 days in the CS group (difference 1.0, 95% CI -0.7, 2.6), while the average MV time was 5.0 days for RS versus 6.0 days for CS. Similar differences were found in the subgroup analysis.
Conclusions: Compared to CS, RS significantly decreases the overall costs in the ICU.
Trial registration: Clinicaltrials.gov NCT00158873.
Figures
References
-
- Gravel NR, Searle NR, Sahab PG, Carrier M. Sedation in critically ill patients: practical recommendations. CNS Drugs. 1999;11:9–22. doi: 10.2165/00023210-199911010-00002. - DOI
-
- Andrews P, Azoulay E, Antonelli M, Brochard L, Brun-Buisson C, Dobb G, Fagon JY, Gerlach H, Groeneveld J, Mancebo J, Metnitz P, Nava S, Pugin J, Pinsky M, Radermacher P, Richard C, Tasker R. Year in review in intensive care medicine, 2005. II. Infection and sepsis, ventilator-associated pneumonia, ethics, haematology and haemostasis, ICU organisation and scoring, brain injury. Intensive Care Med. 2006;32:380–390. doi: 10.1007/s00134-005-0060-y. - DOI - PubMed
-
- Andrews P, Azoulay E, Antonelli M, Brochard L, Brun-Buisson C, De Backer D, Dobb G, Fagon JY, Gerlach H, Groeneveld J, Macrae D, Mancebo J, Metnitz P, Nava S, Pugin J, Pinsky M, Radermacher P, Richard C. Year in review in Intensive Care Medicine, 2006. II. Infections and sepsis, haemodynamics, elderly, invasive and noninvasive mechanical ventilation, weaning, ARDS. Intensive Care Med. 2007;33:214–229. doi: 10.1007/s00134-006-0512-z. - DOI - PMC - PubMed
-
- Mehta S, Hill NS. Noninvasive ventilation. Am J Respir Crit Care Med. 2001;163:540–577. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
