

Estrogen and HER-2 receptor discordance between primary breast cancer and metastasis
- PMID: 21041379
- PMCID: PMC3227913
- DOI: 10.1634/theoncologist.2010-0059
Estrogen and HER-2 receptor discordance between primary breast cancer and metastasis
Abstract
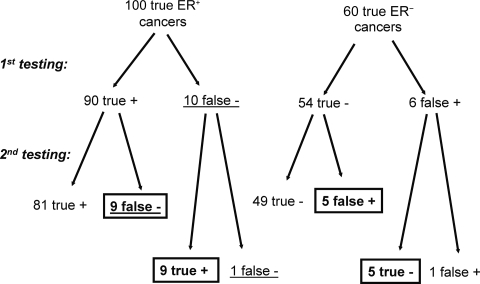
Discordance in estrogen receptor and human epidermal growth factor receptor 2 receptor status between the primary tumor and recurrence is frequently reported in the literature. This is frequently interpreted as evidence for a change in the biology of breast cancer during the course of the disease. This commentary discusses some of the caveats of this interpretation. Discordant receptor results can be caused by any of 3 factors: (a) a genuine switch in the biology of the disease, (b) sampling error in focally receptor-positive cancers, and (c) limited accuracy and reproducibility of receptor assays. The relative contribution of each of these factors to discordant results is unknown. A switch in molecular class between primary and recurrent cancer (or residual cancer after therapy) appears to be a rare event based on the available limited molecular profiling data. Small pockets of strongly focally receptor-positive tumor nests in a larger receptor-negative cancer are also relatively infrequently seen. Discordance resulting from inherent limitations in assay reproducibility is evident from the frequently discordant receptor results even when the same samples are assessed in different laboratories (e.g., central versus local laboratory). A repeat tumor biopsy is clearly justified when it is suspected, on clinical grounds, that the original receptor results may have been false negative or when the diagnosis of metastatic disease is in question. However, routine repeat biopsy for receptor re-evaluation does not necessarily improve diagnostic accuracy and have a potential to harm through a false-negative result. For patients with clinical courses consistent with hormone responsiveness, or with prior positive hormone receptor results, a course of endocrine therapy is reasonable regardless of the most recent hormone receptor assay result.
Conflict of interest statement
The content of this article has been reviewed by independent peer reviewers to ensure that it is balanced, objective, and free from commercial bias. No financial relationships relevant to the content of this article have been disclosed by the authors or independent peer reviewers.
Figures
References
-
- Osborne CK. Heterogeneity in hormone receptor status in primary and metastatic breast cancer. Semin Oncol. 1985;12:317–326. - PubMed
-
- Li BD, Byskosh A, Molteni A, et al. Estrogen and progesterone receptor concordance between primary and recurrent breast cancer. J Surg Oncol. 1994;57:71–77. - PubMed
-
- Spataro V, Price K, Goldhirsch A, et al. Sequential estrogen receptor determinations from primary breast cancer and at relapse: Prognostic and therapeutic relevance. The International Breast Cancer Study Group (formerly Ludwig Group) Ann Oncol. 1992;3:733–740. - PubMed
-
- Simon R, Nocito A, Hübscher T, et al. Patterns of her-2/neu amplification and overexpression in primary and metastatic breast cancer. J Natl Cancer Inst. 2001;93:1141–1146. - PubMed
-
- Holdaway IM, Bowditch JV. Variation in receptor status between primary and metastatic breast cancer. Cancer. 1983;52:479–485. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
