

The Memphis Girls' health Enrichment Multi-site Studies (GEMS): an evaluation of the efficacy of a 2-year obesity prevention program in African American girls
- PMID: 21041593
- PMCID: PMC3052791
- DOI: 10.1001/archpediatrics.2010.196
The Memphis Girls' health Enrichment Multi-site Studies (GEMS): an evaluation of the efficacy of a 2-year obesity prevention program in African American girls
Abstract
Objective: To determine the efficacy of a 2-year obesity prevention program in African American girls.
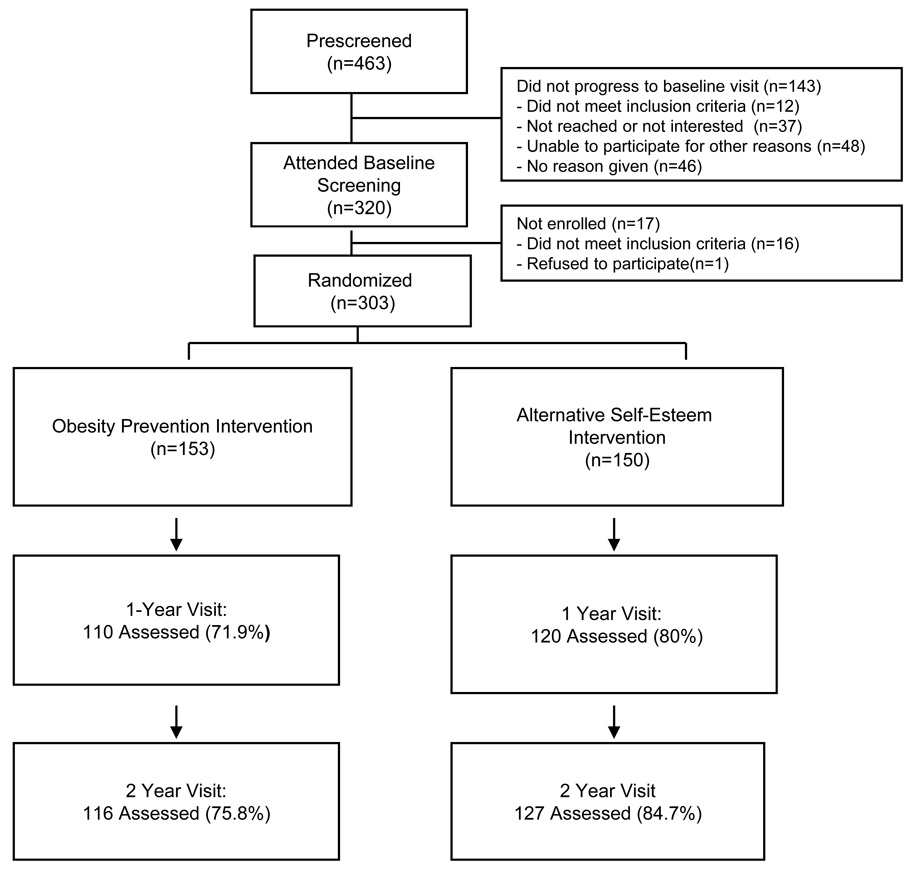
Design: Memphis GEMS (Girls' health Enrichment Multi-site Studies) was a controlled trial in which girls were randomly assigned to an obesity prevention program or alternative intervention.
Setting: Local community centers and YWCAs (Young Women's Christian Associations) in Memphis, Tennessee.
Participants: Girls aged 8 to 10 years (N = 303) who were identified by a parent or guardian as African American and who had a body mass index (BMI) at or higher than the 25th percentile for age or 1 parent with a BMI of 25 or higher.
Interventions: Group behavioral counseling to promote healthy eating and increased physical activity (obesity prevention program) or self-esteem and social efficacy (alternative intervention).
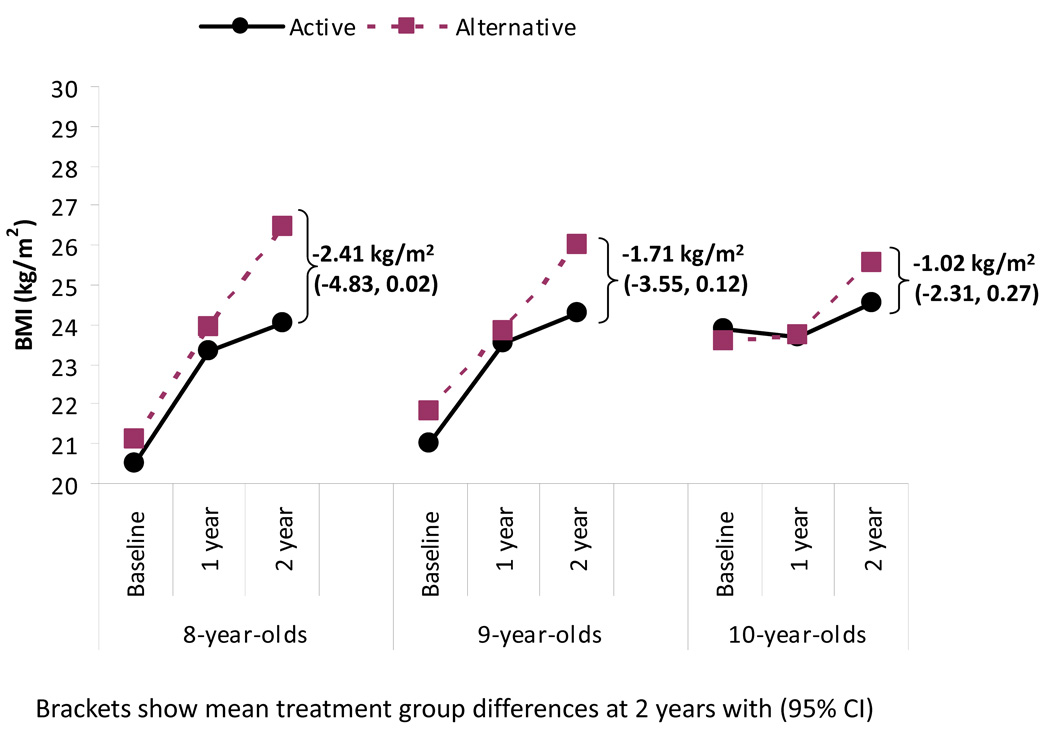
Main outcome measure: The BMI at 2 years.
Results: The BMI increased in all girls with no treatment effect (obesity prevention minus alternative intervention) at 2 years (mean, 0.09; 95% confidence interval [CI], -0.40 to 0.58). Two-year treatment effects in the expected direction were observed for servings per day of sweetened beverages (mean, -0.19; 95% CI, -0.39 to 0.09), water (mean, 0.21; 95% CI, 0.03 to 0.40), and vegetables (mean, 0.15; 95% CI,-0.02 to 0.30), but there were no effects on physical activity. Post hoc analyses suggested a treatment effect in younger girls (P for interaction = .08). The mean BMI difference at 2 years was -2.41 (95% CI, -4.83 to 0.02) in girls initially aged 8 years and -1.02 (95% CI, -2.31 to 0.27) in those initially aged 10 years.
Conclusions: The lack of significant BMI change at 2 years indicates that this intervention alone is insufficient for obesity prevention. Effectiveness may require more explicit behavior change goals and a stronger physical activity component as well as supportive changes in environmental contexts.
Trial registration: ClinicalTrials.gov NCT00000615.
Figures
Comment in
-
Pediatric obesity prevention initiatives: more questions than answers.Arch Pediatr Adolesc Med. 2010 Nov;164(11):1067-9. doi: 10.1001/archpediatrics.2010.186. Arch Pediatr Adolesc Med. 2010. PMID: 21041601 No abstract available.
References
-
- Wang Y, Lobstein T. Worldwide trends in childhood overweight and obesity. Int J Pediatr Obes. 2006;1(1):11–25. - PubMed
-
- Daniels SR, Arnett DK, Eckel RH, et al. Overweight in children and adolescents: pathophysiology, consequences, prevention, and treatment. Circulation. 2005 Apr 19;111(15):1999–2012. - PubMed
-
- Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM. Prevalence of overweight and obesity in the United States, 1999–2004. JAMA. 2006 Apr 5;295(13):1549–1555. - PubMed
-
- Troiano RP, Flegal KM, Kuczmarski RJ, Campbell SM, Johnson CL. Overweight prevalence and trends for children and adolescents. The National Health and Nutrition Examination Surveys, 1963 to 1991. Arch Pediatr Adolesc Med. 1995 Oct;149(10):1085–1091. - PubMed
