

Magnetic resonance imaging of carotid atherosclerotic plaque in clinically suspected acute transient ischemic attack and acute ischemic stroke
- PMID: 21041694
- PMCID: PMC3008416
- DOI: 10.1161/CIRCULATIONAHA.109.866053
Magnetic resonance imaging of carotid atherosclerotic plaque in clinically suspected acute transient ischemic attack and acute ischemic stroke
Abstract
Background: Carotid atherosclerotic plaque rupture is thought to cause transient ischemic attack (TIA) and ischemic stroke (IS). Pathological hallmarks of these plaques have been identified through observational studies. Although generally accepted, the relationship between cerebral thromboembolism and in situ atherosclerotic plaque morphology has never been directly observed noninvasively in the acute setting.
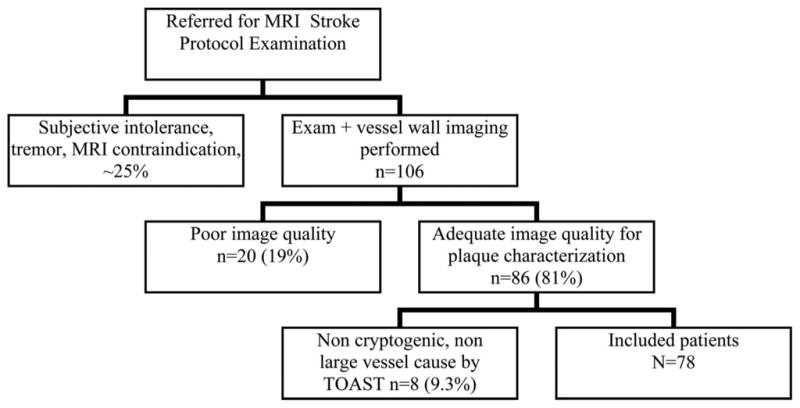
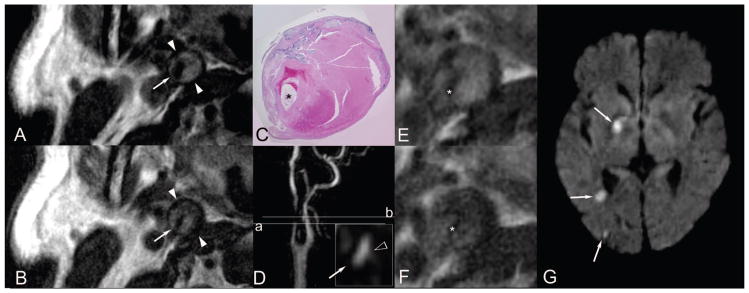
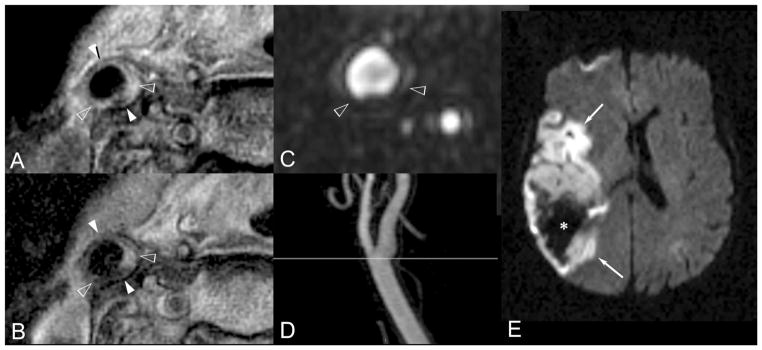
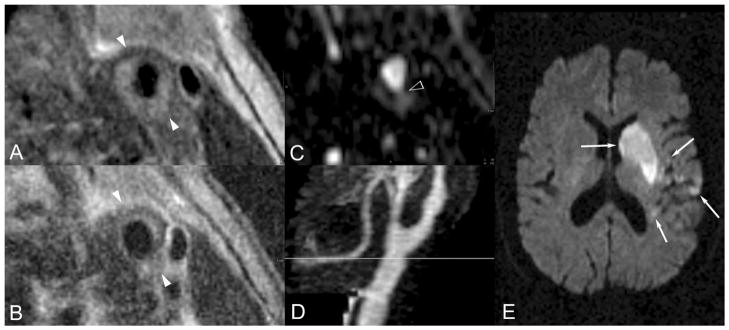
Methods and results: Consecutive acutely symptomatic patients referred for stroke protocol magnetic resonance imaging/angiography underwent additional T1- and T2-weighted carotid bifurcation imaging with the use of a 3-dimensional technique with blood signal suppression. Two blinded reviewers performed plaque gradings according to the American Heart Association classification system. Discharge outcomes and brain magnetic resonance imaging results were obtained. Image quality for plaque characterization was adequate in 86 of 106 patients (81%). Eight TIA/IS patients with noncarotid pathogenesis were excluded, yielding 78 study patients (38 men and 40 women with a mean age of 64.3 years, SD 14.7) with 156 paired watershed vessel/cerebral hemisphere observations. Thirty-seven patients had 40 TIA/IS events. There was a significant association between type VI plaque (demonstrating cap rupture, hemorrhage, and/or thrombosis) and ipsilateral TIA/IS (P<0.001). A multiple logistic regression model including standard Framingham risk factors and type VI plaque was constructed. Type VI plaque was the dominant outcome-associated observation achieving significance (P<0.0001; odds ratio, 11.66; 95% confidence interval, 5.31 to 25.60).
Conclusions: In situ type VI carotid bifurcation region plaque identified by magnetic resonance imaging is associated with ipsilateral acute TIA/IS as an independent identifier of events, thereby supporting the dominant disease pathophysiology.
Figures
References
-
- Executive Committee for the Asymptomatic Carotid Atherosclerosis Study. Endarterectomy for asymptomatic carotid artery stenosis. JAMA. 1995;273:1421–1428. - PubMed
-
- North American Symptomatic Carotid Endarterectomy Trial Collaborators. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. N Engl J Med. 1991;325:445–453. - PubMed
-
- European Carotid Surgery Trialists’ Collaborative Group. MRC European Carotid Surgery Trial: interim results for symptomatic patients with severe (70–99%) or with mild (0–29%) carotid stenosis. Lancet. 1991;337:1235–1243. - PubMed
-
- Glagov S, Weisenberg E, Zarins CK, Stankunavicius R, Kolettis GJ. Compensatory enlargement of human atherosclerotic coronary arteries. N Engl J Med. 1987;316:1371–1375. - PubMed
-
- Ambrose JA, Tannenbaum MA, Alexopoulos D, Hjemdahl-Monsen CE, Leavy J, Weiss M, Borrico S, Gorlin R, Fuster V. Angiographic progression of coronary artery disease and the development of myocardial infarction. J Am Coll Cardiol. 1988;12:56–62. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
