

Central modulation of pain
- PMID: 21041960
- PMCID: PMC2964993
- DOI: 10.1172/JCI43766
Central modulation of pain
Abstract
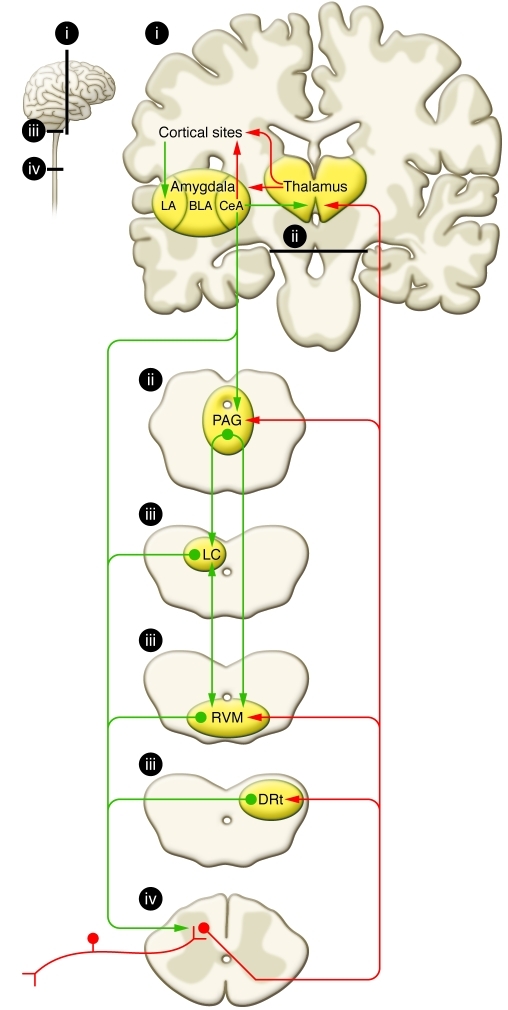
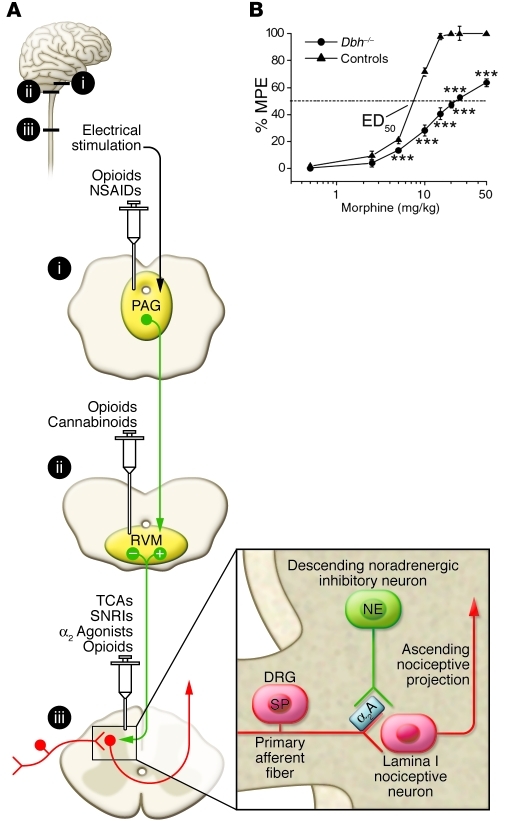
It has long been appreciated that the experience of pain is highly variable between individuals. Pain results from activation of sensory receptors specialized to detect actual or impending tissue damage (i.e., nociceptors). However, a direct correlation between activation of nociceptors and the sensory experience of pain is not always apparent. Even in cases in which the severity of injury appears similar, individual pain experiences may vary dramatically. Emotional state, degree of anxiety, attention and distraction, past experiences, memories, and many other factors can either enhance or diminish the pain experience. Here, we review evidence for "top-down" modulatory circuits that profoundly change the sensory experience of pain.
Figures
References
-
- Bingel U, Tracey I. Imaging CNS modulation of pain in humans. Physiology (Bethesda). 2008;23(3):371–380. - PubMed
-
- Fields HL, Basbaum AI, Heinricher MM. Central nervous system mechanisms of pain modulation. In: McMahon S, Koltzenburg M, eds.Textbook of Pain . 5th ed. Burlington, Massachusetts, USA: Elsevier Health Sciences; 2005:125–142.
-
- Beecher HK. The powerful placebo. J Am Med Assoc. 1955;159(17):1602–1606. - PubMed
-
- Levine JD, Gordon NC, Fields HL. The mechanism of placebo analgesia. Lancet. 1978;2(8091):654–657. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
