

Perspectives on anaphylaxis epidemiology in the United States with new data and analyses
- PMID: 21042959
- PMCID: PMC3020316
- DOI: 10.1007/s11882-010-0154-7
Perspectives on anaphylaxis epidemiology in the United States with new data and analyses
Abstract
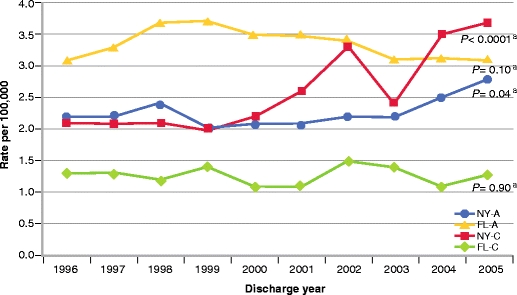
Anaphylaxis incidence rates and time trends in the United States have been reported using different data sources and selection methods. Larger studies using diagnostic coding have inherent limitations in sensitivity and specificity. In contrast, smaller studies using chart reviews, including reports from single institutions, have better case characterization but suffer from reduced external validity due to their restricted nature. Increasing anaphylaxis hospitalization rates since the 1990s have been reported abroad. However, we report no significant overall increase in the United States. There have been several reports of increasing anaphylaxis rates in northern populations in the United States, especially in younger people, lending support to the suggestion that higher anaphylaxis rates occur at higher latitudes. We analyzed anaphylaxis hospitalization rates in comparably sized northern (New York) and southern (Florida) states and found significant time trend differences based on age. This suggests that the relationship of latitude to anaphylaxis incidence is complex.
Figures
References
-
- An epidemiologic study of severe anaphylactic and anaphylactoid reactions among hospital patients: methods and overall risks. The International Collaborative Study of Severe Anaphylaxis. Epidemiology 1998, 9:141–146. - PubMed
-
- Moneret-Vautrin DA, Kanny G, Parisot L. First survey from the “Allergy Vigilance Network”: life-threatening food allergies in France. Allerg Immunol (Paris) 2002;34:194–198. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
