

Symptoms predicting remission after divalproex augmentation with olanzapine in partially nonresponsive patients experiencing mixed bipolar I episode: a post-hoc analysis of a randomized controlled study
- PMID: 21044339
- PMCID: PMC2987872
- DOI: 10.1186/1756-0500-3-276
Symptoms predicting remission after divalproex augmentation with olanzapine in partially nonresponsive patients experiencing mixed bipolar I episode: a post-hoc analysis of a randomized controlled study
Abstract
Background: Rating scale items in a 6-week clinical trial of olanzapine versus placebo augmentation in patients with mixed bipolar disorder partially nonresponsive to ≥14 days of divalproex monotherapy were analyzed to characterize symptom patterns that could predict remission. At baseline, the two treatment groups were similar.
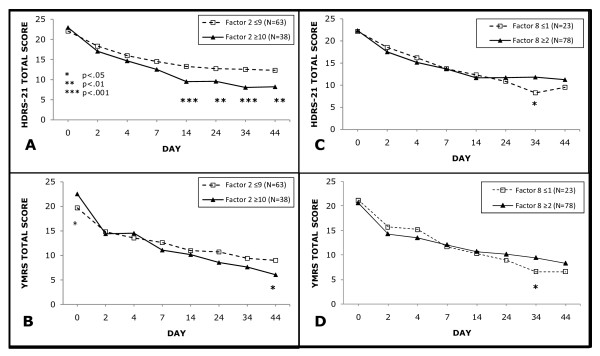
Findings: Factor analysis with Varimax rotation was performed post hoc on baseline items of the 21-Item Hamilton Depression Rating Scale (HDRS-21) and Young Mania Rating Scale (YMRS). Backwards-elimination logistic regression ascertained factors predictive of protocol-defined endpoint remission (HDRS-21 score ≤ 8 and YMRS score ≤ 12) with subsequent determination of optimally predictive factor score cutoffs.Factors for Psychomotor activity (YMRS items for elevated mood, increased motor activity, and increased speech and HDRS-21 agitation item) and Guilt/Suicidality (HDRS-21 items for guilt and suicidality) significantly predicted endpoint remission in the divalproex+olanzapine group. No factor predicted remission in the divalproex+placebo group. Patients in the divalproex+olanzapine group with high pre-augmentation psychomotor activity (scores ≥10) were more likely to remit compared to those with lower psychomotor activity (odds ratio [OR] = 3.09, 95% confidence interval [CI] = 1.22-7.79), and patients with marginally high Guilt/Suicidality (scores ≥2) were less likely to remit than those with lower scores (OR = 0.37, 95% CI = 0.13-1.03). Remission rates for divalproex+placebo vs. divalproex+olanzapine patients with high psychomotor activity scores were 22% vs. 45% (p = 0.08) and 33% vs. 48% (p = 0.29) for patients with low Guilt/Suicidality scores.
Conclusions: Patients who were partially nonresponsive to divalproex treatment with remaining high vs. low psychomotor activity levels or minimal vs. greater guilt/suicidality symptoms were more likely to remit with olanzapine augmentation.
Trial registration: ClinicalTrials.gov; http://clinicaltrials.gov/ct2/show/NCT00402324?term=NCT00402324&rank=1, Identifier: NCT00402324.
Figures
References
-
- Suppes T, Brown E, Schuh LM, Baker RW, Tohen M. Rapid versus non-rapid cycling as a predictor of response to olanzapine and divalproex sodium for bipolar mania and maintenance of remission: post hoc analyses of 47-week data. J Affect Disord. 2005;89:69–77. doi: 10.1016/j.jad.2005.07.011. - DOI - PubMed
-
- Ketter TA, Houston JP, Adams DH, Risser RC, Meyers AL, Williamson DJ, Tohen M. Differential efficacy of olanzapine and lithium in preventing manic or mixed recurrence in patients with bipolar I disorder based on number of previous manic or mixed episodes. J Clin Psychiatry. 2006;67:95–101. doi: 10.4088/JCP.v67n0113. - DOI - PubMed
-
- Perlis RH, Ostacher MJ, Patel JK, Marangell LB, Zhang H, Wisniewski SR, Ketter TA, Miklowitz DJ, Otto MW, Gyulai L. et al. Predictors of recurrence in bipolar disorder: primary outcomes from the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) Am J Psychiatry. 2006;163:217–224. doi: 10.1176/appi.ajp.163.2.217. - DOI - PubMed
-
- Keller MB, Lavori PW, Kane JM, Gelenberg AJ, Rosenbaum JF, Walzer EA, Baker LA. Subsyndromal symptoms in bipolar disorder. A comparison of standard and low serum levels of lithium. Arch Gen Psychiatry. 1992;49:371–376. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
