

Clinical target volume delineation in glioblastomas: pre-operative versus post-operative/pre-radiotherapy MRI
- PMID: 21045069
- PMCID: PMC3473876
- DOI: 10.1259/bjr/10315979
Clinical target volume delineation in glioblastomas: pre-operative versus post-operative/pre-radiotherapy MRI
Abstract
Objectives: Delineation of clinical target volume (CTV) is still controversial in glioblastomas. In order to assess the differences in volume and shape of the radiotherapy target, the use of pre-operative vs post-operative/pre-radiotherapy T(1) and T(2) weighted MRI was compared.
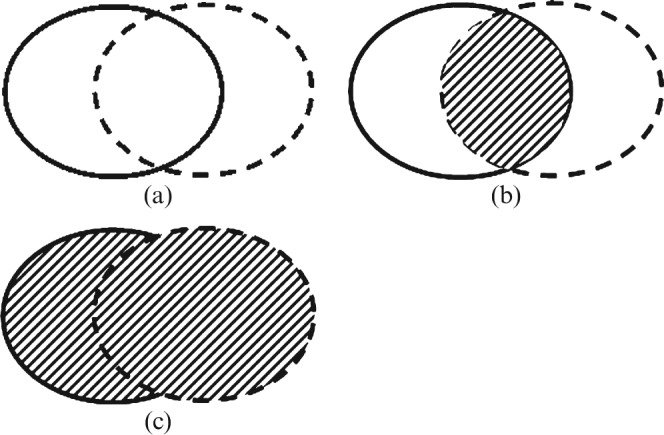
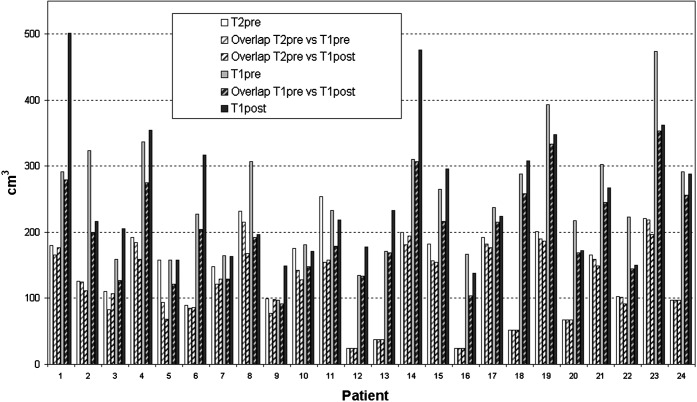
Methods: 4 CTVs were delineated in 24 patients pre-operatively and post-operatively using T(1) contrast-enhanced (T1(PRE)CTV and T1(POST)CTV) and T(2) weighted images (T2(PRE)CTV and T2(POST)CTV). Pre-operative MRI examinations were performed the day before surgery, whereas post-operative examinations were acquired 1 month after surgery and before chemoradiation. A concordance index (CI) was defined as the ratio between the overlapping and composite volumes.
Results: The volumes of T1(PRE)CTV and T1(POST)CTV were not statistically different (248 ± 88 vs 254 ± 101), although volume differences >100 cm(3) were observed in 6 out of 24 patients. A marked increase due to tumour progression was shown in three patients. Three patients showed a decrease because of a reduced mass effect. A significant reduction occurred between pre-operative and post-operative T(2) volumes (139 ± 68 vs 78 ± 59). Lack of concordance was observed between T1(PRE)CTV and T1(POST)CTV (CI = 0.67 ± 0.09), T2(PRE)CTV and T2(POST)CTV (CI = 0.39 ± 0.20) and comparing the portion of the T1(PRE)CTV and T1(POST)CTV not covered by that defined on T2(PRE)CTV images (CI = 0.45 ± 0.16 and 0.44 ± 0.17, respectively).
Conclusion: Using T(2) MRI, huge variations can be observed in peritumoural oedema, which are probably due to steroid treatment. Using T(1) MRI, brain shifts after surgery and possible progressive enhancing lesions produce substantial differences in CTVs. Our data support the use of post-operative/pre-radiotherapy T(1) weighted MRI for planning purposes.
Figures
References
-
- Stupp R, Hegi ME, Gilbert MR, Chakravarti A. Chemoradiotherapy in malignant glioma: standard of care and future directions. J Clin Oncol 2007;25:4127–36 - PubMed
-
- Laperriere N, Zuraw L, Cairncross G. Cancer Care Ontario Practice Guidelines Initiative Neuro-Oncology Disease Site Group. Radiotherapy for newly diagnosed malignant glioma in adults: a systematic review. Radiother Oncol 2002;64:259–73 - PubMed
-
- Baumert BG, Brada M, Bernier J, Kortmann RD, Dehing-Oberije C, Collette L, et al. EORTC 22972–26991/MRC BR10 trial: fractionated stereotactic boost following conventional radiotherapy of high grade gliomas. Clinical and quality-assurance results of the stereotactic boost arm. Radiother Oncol 2008;88:163–72 - PubMed
-
- Buatti J, Ryken TC, Smith MC, Sneed P, Suh JH, Mehta M, et al. Radiation therapy of pathologically confirmed newly diagnosed glioblastoma in adults. J Neurooncol 2008;89:313–37 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
