

Change in disability after hospitalization or restricted activity in older persons
- PMID: 21045098
- PMCID: PMC3124926
- DOI: 10.1001/jama.2010.1568
Change in disability after hospitalization or restricted activity in older persons
Erratum in
- JAMA. 2011 Apr 6;305(13):1301
Abstract
Context: Disability among older persons is a complex and highly dynamic process, with high rates of recovery and frequent transitions between states of disability. The role of intervening illnesses and injuries (ie, events) on these transitions is uncertain.
Objectives: To evaluate the relationship between intervening events and transitions among states of no disability, mild disability, severe disability, and death and to determine the association of physical frailty with these transitions.
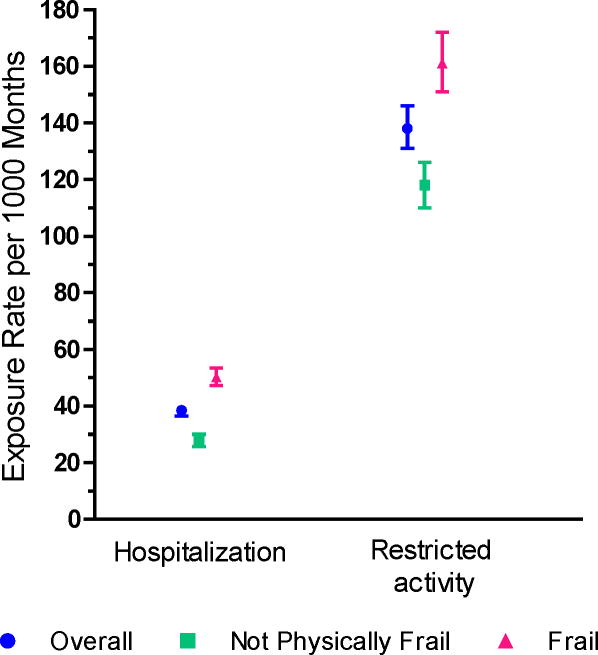
Design, setting, and participants: Prospective cohort study conducted in greater New Haven, Connecticut, from March 1998 to December 2008 of 754 community-living persons aged 70 years or older who were nondisabled at baseline in 4 essential activities of daily living: bathing, dressing, walking, and transferring. Telephone interviews were completed monthly for more than 10 years to assess disability and ascertain exposure to intervening events, which included illnesses and injuries leading to either hospitalization or restricted activity. Physical frailty (defined as gait speed >10 seconds on the rapid gait test) was assessed every 18 months through 108 months.
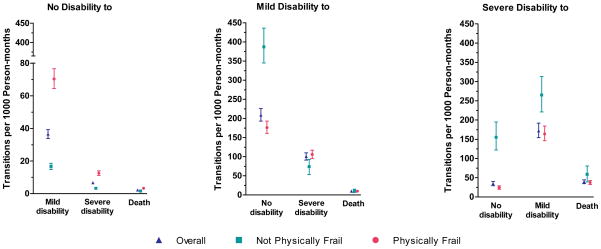
Main outcome measure: Transitions between no disability, mild disability, and severe disability and 3 transitions from each of these states to death, evaluated each month.
Results: Hospitalization was strongly associated with 8 of the 9 possible transitions, with increased multivariable hazard ratios (HRs) as high as 168 (95% confidence interval [CI], 118-239) for the transition from no disability to severe disability and decreased HRs as low as 0.41 (95% CI, 0.30-0.54) for the transition from mild disability to no disability. Restricted activity also increased the likelihood of transitioning from no disability to both mild and severe disability (HR, 2.59; 95% CI, 2.23-3.02; and HR, 8.03; 95% CI, 5.28-12.21), respectively, and from mild disability to severe disability (HR, 1.45; 95% CI, 1.14-1.84), but was not associated with recovery from mild or severe disability. For all 9 transitions, the presence of physical frailty accentuated the associations of the intervening events. For example, the absolute risk of transitioning from no disability to mild disability within 1 month after hospitalization for frail individuals was 34.9% (95% CI, 34.5%-35.3%) vs 4.9% (95% CI, 4.7%-5.1%) for nonfrail individuals. Among the possible reasons for hospitalization, fall-related injury conferred the highest likelihood of developing new or worsening disability.
Conclusions: Among older persons, particularly those who were physically frail, intervening illnesses and injuries greatly increased the likelihood of developing new or worsening disability. Only the most potent events, ie, those leading to hospitalization, reduced the likelihood of recovery from disability.
Figures
References
-
- Fried LP, Guralnik JM. Disability in older adults: evidence regarding significance, etiology, and risk. J Am Geriatr Soc. 1997;45:92–100. - PubMed
-
- Katz S, Branch LG, Branson MH, Papsidero JA, Beck JC, Greer DS. Active life expectancy. N Engl J Med. 1983;309:1218–1224. - PubMed
-
- Manton KG, Stallard E, Liu K. Forecasts of active life expectancy: policy and fiscal implications. J Gerontol. 1993;48(Spec No):11–26. - PubMed
-
- Campbell AJ, Buchner DM. Unstable disability and the fluctuations of frailty. Age Ageing. 1997;26:315–318. - PubMed
