

The utility and cost of routine follow-up procedures in the surveillance of ovarian and primary peritoneal carcinoma: a 16-year institutional review
- PMID: 21045830
- PMCID: PMC2994227
- DOI: 10.1038/sj.bjc.6605963
The utility and cost of routine follow-up procedures in the surveillance of ovarian and primary peritoneal carcinoma: a 16-year institutional review
Abstract
Background: The purpose of this study was to evaluate the number of ovarian cancer and primary peritoneal cancer (PPC) progressive disease cases identified via routine follow-up procedures and the corresponding cost throughout a 16-year period at a single medical institution.
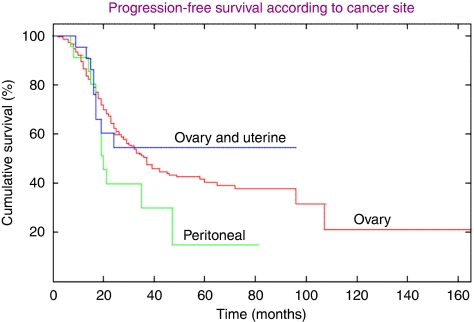
Methods: Previously undiagnosed epithelial ovarian (n=241), PPC (n=23), and concurrent ovarian and uterine (n=24) cancer patients were treated and then followed via CA-125, imaging (e.g., CT scan, chest X-ray), physical examination and vaginal cytology.
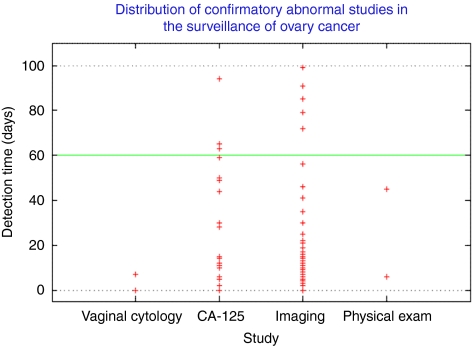
Results: In the group of 287 patients, there were 151 cases of disease progression. Serial imaging detected the highest number of progressive disease cases (66 initial and 45 confirmatory diagnoses), but the cost was rather high ($13,454 per patient recurrence), whereas CA-125 testing (74 initial and 20 corroborative diagnoses) was the least expensive ($3,924) per recurrent diagnosis. The total cost of surveillance during the 16-year period was nearly $2,400,000.
Conclusion: Ultimately, serial imaging and the CA-125 assay detected the highest number of ovarian cancer and PCC progressive disease cases in comparison to physical examination and vaginal cytology, but nevertheless, all of the procedures were conducted at a considerable financial expense.
Figures
References
-
- Aletti GD, Powless C, Bakkum-Gamez J, Wilson TO, Podratz KC, Cliby WA (2009) Pattern of retroperitoneal dissemination of primary peritoneum cancer: basis for rational use of lymphadenectomy. Gynecol Oncol 114: 32–36 - PubMed
-
- Bast Jr RC, Brewer M, Zou C, Hernandez MA, Daley M, Ozols R, Lu K, Lu Z, Badgwell D, Mills GB, Skates S, Zhang Z, Chan D, Lokshin A, Yu Y (2007) Prevention and early detection of ovarian cancer: mission impossible? Recent Results Cancer Res 174: 91–100 - PubMed
-
- Berek JS, Trope C, Vergote I (1999) Surgery during chemotherapy and at relapse of ovarian cancer. Ann Oncol 10: 3–7 - PubMed
-
- Bristow RE, Purinton SC, Santillan A, Diaz-Montes TP, Gardner GJ, Giuntoli II RL (2006) Cost-effectiveness of routine vaginal cytology for endometrial cancer surveillance. Gynecol Oncol 103: 709–713 - PubMed
-
- Casey AC, Park M, Holschneider C, Bozuk M, Punyasavatsut M, Montz FJ (1996) Apical vaginal recurrence of ovarian carcinoma: presentation, treatment and survival. Int J Gynecol Cancer 6: 200–204
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
