

Restricted Diffusion of Pus in the Subarachnoid Space: MRSA Meningo-Vasculitis and Progressive Brainstem Ischemic Strokes - A Case Report
- PMID: 21045937
- PMCID: PMC2968771
- DOI: 10.1159/000319691
Restricted Diffusion of Pus in the Subarachnoid Space: MRSA Meningo-Vasculitis and Progressive Brainstem Ischemic Strokes - A Case Report
Abstract
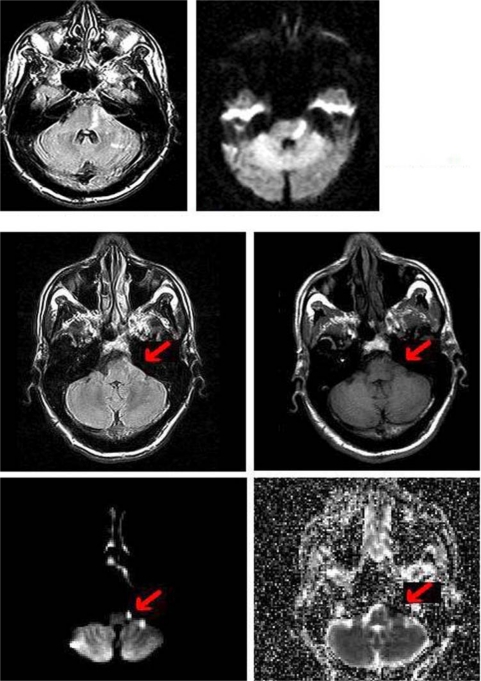
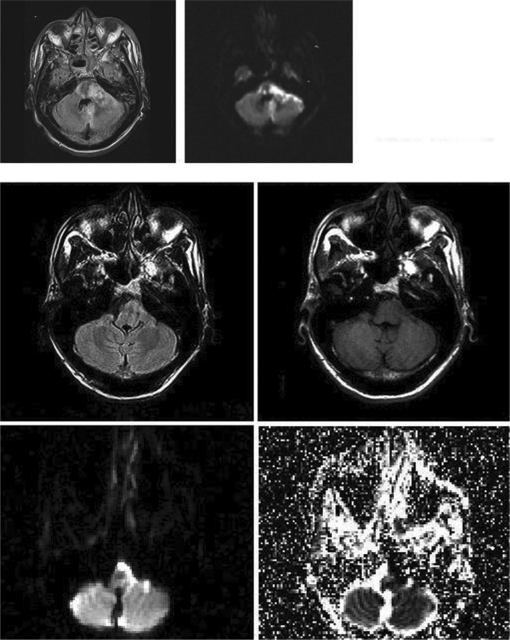
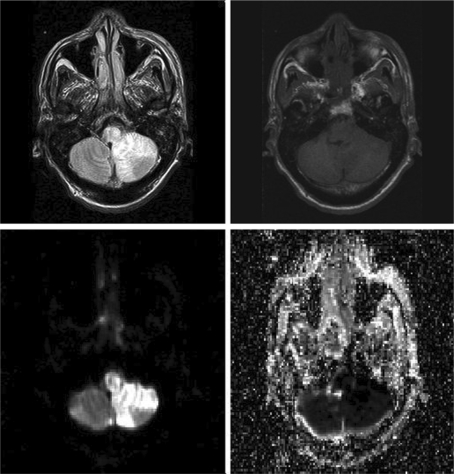
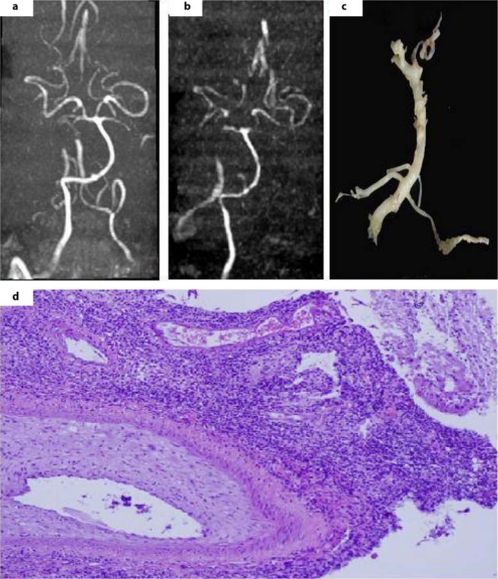
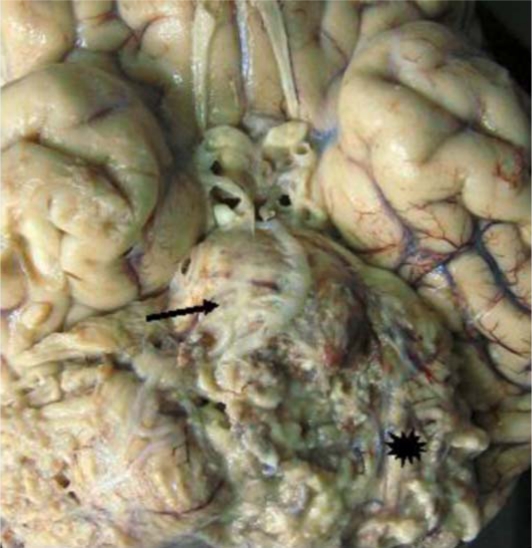
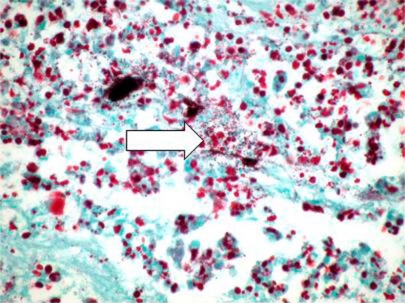
Extra-axial restriction on diffusion weighted imaging (DWI) is an unusual finding on brain magnetic resonance imaging (MRI). Intra-axial restriction on DWI, however, is common, and can represent brain parenchymal infarction, tumor, abscess, or toxic-metabolic process. The infrequency of extra-axial DWI restriction and the paucity of clinico-pathological correlation in the literature limit its differential diagnosis. Scant case reports suggest that extra-axial DWI restriction could be a lymphoma, neurenteric cyst, or, in one patient, subdural empyema [1,2,3]. We postulate that pus formation must be excluded first, because it can provoke an aggressive meningo-vasculitis with rapidly fatal, intra-axial infarctions. Our patient was a 45-year-old man, presenting to our hospital with left facial droop and right (contralateral) arm and leg weakness. Initial MRI revealed DWI restriction in the left lateral pons, consistent with a classic Millard-Gubler stroke. Also noted was a subtle, extra-axial area of curvilinear diffusion restriction in the left cerebellar-pontine angle's subarachnoid space. Days later, the patient had a headache, and repeat MRI revealed extension of the two DWI lesions - both the intra-axial pontine infarction and the extra-axial area of restricted diffusion in the subarachnoid space. The patient became comatose, a third MRI revealed more extensive DWI restrictions, and he expired despite aggressive care. Autopsy revealed massive brainstem infarcts, a thick lymphoplasmacytic infiltrate, copious Gram-Positive cocci (likely MRSA) and arteries partially occluded with fibrointimal proliferation. This emphasizes the concept that extra-axial DWI restriction can represent pus development in the subarachnoid space - a radiographic marker to identify a patient at risk for demise due to septic, meningo-vasculitic infarctions.
Figures
References
-
- Zacharia TT, Law M, Naidich TP, Leeds NE. Central nervous system lymphoma characterization by diffusion-weighted imaging and MR spectroscopy. J Neuroimaging. 2008;18:411–417. - PubMed
-
- Jan W, Zimmerman RA, Bilaniuk LT, Hunter JV, Simon EM, Haselgrove J. Diffusion-weighted imaging in acute bacterial meningitis in infancy. Neuroradiology. 2003;45:634–639. - PubMed
-
- Lee SB, Jones LK, Gianinni C. Brainstem infarcts as an early manifestation of Streptococcus angisnosus meningitis. Neurocrit Care. 2005;3:157–160. - PubMed
-
- Perry JR, Bilbao JM, Gray T. Fatal basilar vasculopathy complicationg bacterial meningitis. Stroke. 1992;23:1175–1178. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
