

Modification of the sinus tarsi approach for open reduction and plate fixation of intra-articular calcaneus fractures: the limits of proximal extension based upon the vascular anatomy of the lateral calcaneal artery
- PMID: 21045990
- PMCID: PMC2958289
Modification of the sinus tarsi approach for open reduction and plate fixation of intra-articular calcaneus fractures: the limits of proximal extension based upon the vascular anatomy of the lateral calcaneal artery
Abstract
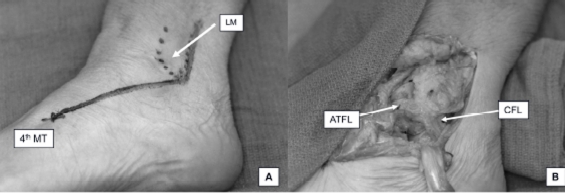
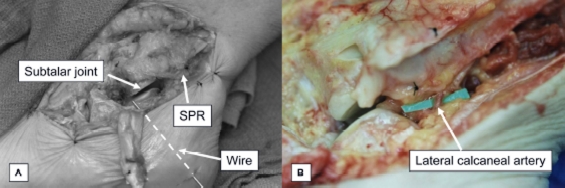
The treatment of displaced calcaneal fractures remains controversial. Early surgical management to restore articular congruence and the structural function of the calcaneus is widely accepted as the best way to avoid the negative consequences of malunion. Concerns remain however regarding the best approach for reducing and maintaining reduction of these complex fractures, while minimizing the risk of surgical complications. The potential for serious wound complications is a major concern, particularly breakdown of the lateral calcaneal skin flap with the extensile lateral approach. Various approaches have been developed to try and balance the need for direct reduction of the articular surface while minimizing the potential for wound complications. Palmer originally described a laterally based approach through the sinus tarsi for direct visualization of the articular surface for reduction. He and others have found this approach to be useful and reasonably safe. At times, however, it may be necessary to extend the limits of a small incision over the sinus tarsi to treat adjacent fractures or to aid reduction in more complex fractures. In addition, a limited sinus tarsi incision without elevation of the lateral calcaneal skin flap does not allow for plate fixation, a notable advantage of the extensile lateral approach, particularly in gaining reduction of the body of the calcaneus. The authors have used an extended sinus tarsi approach to include placement of plate percutaneously beneath the lateral calcaneal skin flap through a sinus tarsi approach, and to treat adjacent fractures and soft tissue injuries. A clinical series of 13 patients (including 7 chronic smokers and 1 with diabetes and vascular disease) with closed displaced intra-articular calcaneal fractures (Sanders types II and III) were treated by open reduction and internal fixation via this approach. Adjacent fractures were treated through the same incision. Two patients developed wound complications. No wound complications occurred in smokers. The vascular anatomy of the lateral calcaneal artery related to this approach was also studied with 16 cadaver legs. The lateral calcaneal artery (LCA) passed within 2 mm of the superior border of floor of the Superior Peroneal Retinaculum (SPR) at the midline of the peroneal sheath. By avoiding dissection through the deep portion of the SPR, the lateral calcaneal artery can be protected, thus preserving the blood supply to the lateral calcaneal skin flap.
Figures
References
-
- Essex-Lopresti P. The mechanism, reduction technique, and results in fractures of the os calcis. Br J Surg. 1952;39:395–419. - PubMed
-
- Letournel E. Open treatment of acute calcaneal fractures. Clin Orthop Relat Res. 1993:60–67. - PubMed
-
- Palmer I. The mechanism and treatment of fractures of the calcaneus; open reduction with the use of cancelhus grafts. J Bone Joint Surg Am. 1948;30A:2–8. - PubMed
-
- Zwipp H, Tscherne H, Wulker N. [Osteosynthesis of dislocated intraarticular calcaneus fractures] Unfallchirurg. 1988;91:507–515. - PubMed
-
- Gould N. Lateral approach to the os calcis. Foot Ankle. 1984;4:218–220. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials