

The spectrum of gnathic osteosarcoma: caveats for the clinician and the pathologist
- PMID: 21046296
- PMCID: PMC3037463
- DOI: 10.1007/s12105-010-0218-y
The spectrum of gnathic osteosarcoma: caveats for the clinician and the pathologist
Abstract
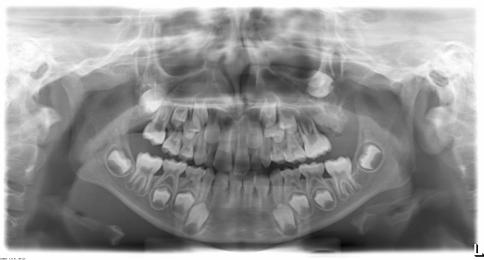
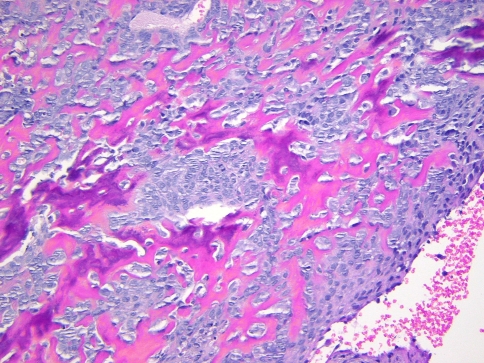
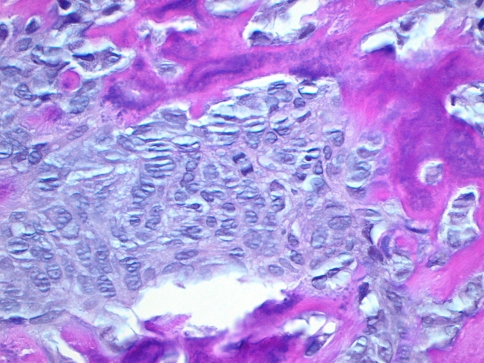
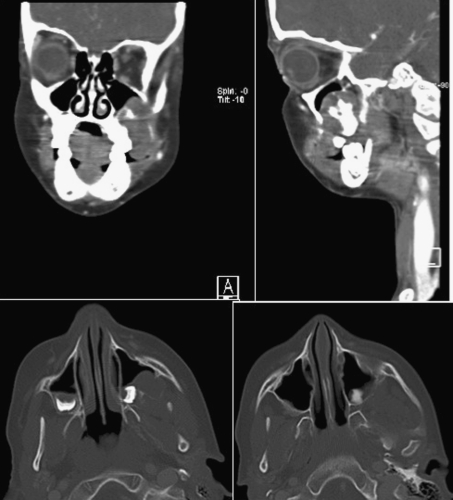
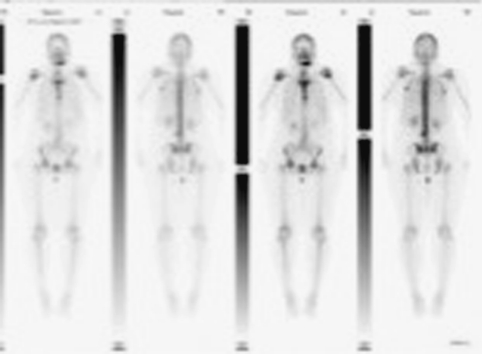
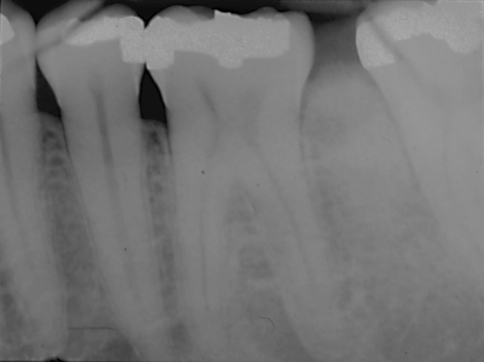
Seven expansile jaw lesions in patients ranging from 7 to 63 years are presented to illustrate diagnostic and management issues pertaining to cases ultimately proven to be gnathic osteosarcoma (GO). Six of the cases in our series were low-grade osteoblastic and one high-grade chondroblastic. None of our cases exhibited the characteristic "sunburst" radiopaque appearance described for GO. All of our cases displayed cortical expansion and one showed development of diastema. Two occurred in the maxilla and five in the mandible. Two of the patients with mandibular lesions presented initially with pain; all other patients were asymptomatic. Lack of pain resulted in a delay in diagnosis due to postponement of consultation or biopsy. Two cases underwent initial shallow non-representative biopsies, requiring a second biopsy for definitive diagnosis, further delaying treatment. Those biopsies were initially interpreted as pyogenic granuloma and peripheral ossifying fibroma, respectively. GO should always be considered in the differential diagnosis of expansile jaw lesions. Bone biopsies of lesions exhibiting pain and expansion of cortical plates should include medullary bone in order to minimize sampling error. In addition, all rapidly growing or painful exophytic bone lesions, and presumed soft tissue lesions that may involve underlying bone, should be examined histopathologically, and receive clinical and radiographic follow-up until complete resolution or healing is evident, regardless of the diagnosis. Based on the positive outcomes of the patients in our series, the prognosis of GO appears to be relatively favorable when compared to other sarcomas and osteosarcomas of long bones.
Figures







References
-
- Fletcher CDM, Unni KK, Mertens F, editors. World Health Organization classification of tumors. Pathology and genetics of tumors of soft tissue and bone. Lyon: IARC Press; 2002.
-
- Barnes L, Eveson JW, Reichart P, Sidransky D, editors. World Health Organization classification of tumours. Pathology and genetics of head and neck tumours. Lyon: IARC Press; 2005.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
