

Effect of oral β-blocker on short and long-term mortality in patients with acute respiratory failure: results from the BASEL-II-ICU study
- PMID: 21047406
- PMCID: PMC3219994
- DOI: 10.1186/cc9317
Effect of oral β-blocker on short and long-term mortality in patients with acute respiratory failure: results from the BASEL-II-ICU study
Abstract
Introduction: Acute respiratory failure (ARF) is responsible for about one-third of intensive care unit (ICU) admissions and is associated with adverse outcomes. Predictors of short- and long-term outcomes in unselected ICU-patients with ARF are ill-defined. The purpose of this analysis was to determine predictors of in-hospital and one-year mortality and assess the effects of oral beta-blockers in unselected ICU patients with ARF included in the BASEL-II-ICU study.
Methods: The BASEL II-ICU study was a prospective, multicenter, randomized, single-blinded, controlled trial of 314 (mean age 70 (62 to 79) years) ICU patients with ARF evaluating impact of a B-type natriuretic peptide- (BNP) guided management strategy on short-term outcomes.
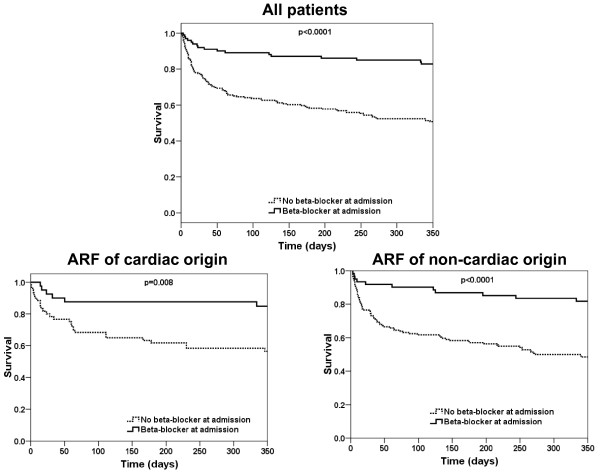
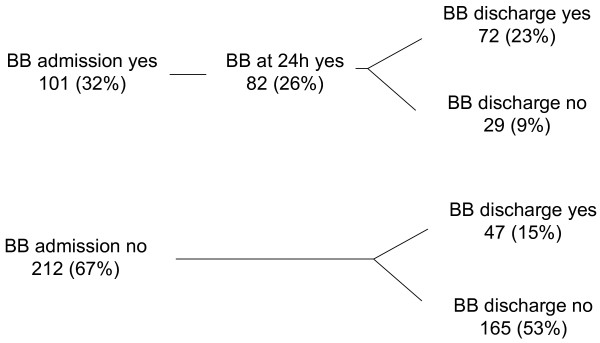
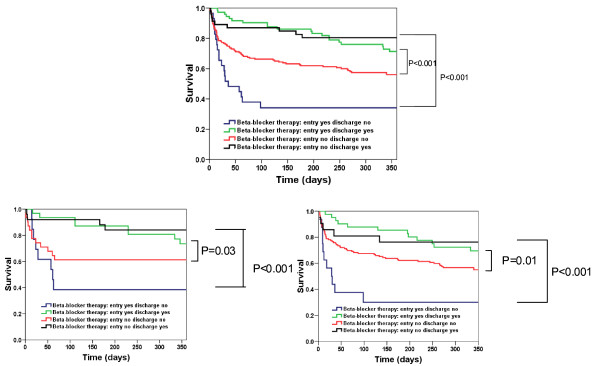
Results: In-hospital mortality was 16% (51 patients) and one-year mortality 41% (128 patients). Multivariate analysis assessed that oral beta-blockers at admission were associated with a lower risk of both in-hospital (HR 0.33 (0.14 to 0.74) P = 0.007) and one-year mortality (HR 0.29 (0.16 to 0.51) P = 0.0003). Kaplan-Meier analysis confirmed the lower mortality in ARF patients when admitted with oral beta-blocker and further shows that the beneficial effect of oral beta-blockers at admission holds true in the two subgroups of patients with ARF related to cardiac or non-cardiac causes. Kaplan-Meier analysis also shows that administration of oral beta-blockers before hospital discharge gives striking additional beneficial effects on one-year mortality.
Conclusions: Established beta-blocker therapy appears to be associated with a reduced mortality in ICU patients with acute respiratory failure. Cessation of established therapy appears to be hazardous. Initiation of therapy prior to discharge appears to confer benefit. This finding was seen regardless of the cardiac or non-cardiac etiology of respiratory failure.
Trial registration: clinicalTrials.gov Identifier: NCT00130559.
Figures
Comment in
-
Beta 2 antagonism in acute respiratory failure.Crit Care. 2010;14(6):1012. doi: 10.1186/cc9359. Epub 2010 Dec 20. Crit Care. 2010. PMID: 21176173 Free PMC article. Review.
References
-
- Luhr OR, Antonsen K, Karlsson M, Aardal S, Thorsteinsson A, Frostell CG, Bonde J. Incidence and mortality after acute respiratory failure and acute respiratory distress syndrome in Sweden, Denmark, and Iceland. The ARF Study Group. Am J Respir Crit Care Med. 1999;159:1849–1861. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
